
Your erection probably isn't as good as it used to be. That's not a failure — it's biology. But it is worth doing something about.
This is a series of three articles Part 1 "Why your Erection is a Window Into Your Heart?" , Part II "How to improve erections?" and Part III "How to do breathwork and core exercises for better sex?"
The Two-Minute Version
Your body runs a nightly erection cycle that maintains penile tissue health. As you age, those erections become less frequent and less firm — and so does your waking function.
The Erectile Hardness Score gives you a simple way to track where you sit. Others may want to explore new devices for tracking including Adam Sensor or FirmTech. If you were once a 4 and you're now a comfortable 3, you've already started losing ground.
PDE5 inhibitors and vacuum erection devices are the most evidence-backed tools for both treatment and prevention. Radiofrequency therapy (Vertica) is showing early promise; PRP is interesting but still experimental. Shockwave therapy sits somewhere in between.
But underneath all of it, kegel exercises and core strength are the non-negotiable foundation. They cost nothing, they have no side effects, and they support everything else you might do.
Start before it's a problem, and it's far less likely to become one.
Here's a scenario that plays out in consulting rooms every week: a bloke in his mid-40s comes in for something unrelated — a blood pressure check, a dodgy knee, a skin check. Somewhere in the conversation, almost as an afterthought, he mentions things aren't quite what they used to be in the bedroom. "It's fine," he says. "It still works. It's just... not the same."
He's right. It's not the same. And the fact that he's normalised a decline he would have noticed immediately ten years ago is actually the most important part of the story.
Your Body Already Runs a Nightly Self-Test
Before we talk about what to do, it's worth understanding what your body is already doing to maintain itself — and what it's been trying to tell you.
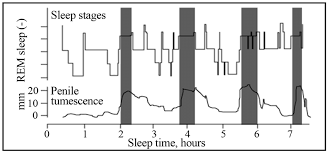
Nocturnal penile tumescence (NPT) — the medical term for overnight erections — occurs spontaneously during REM sleep in all sexually healthy men, typically 3-5x times per night. These aren't triggered by sexual dreams. They're driven by shifts in the autonomic nervous system during deep sleep, when the parasympathetic nervous system takes over from the sympathetic (fight-or-flight) system, promoting blood vessel relaxation and increased blood flow to the penis.
What you experience as "morning wood" is simply the last of these erections — the one you wake up during.
Here's why it matters: these erections deliver oxygen-rich blood to penile tissue, helping keep it healthy and elastic. They're not random — they're your body's built-in maintenance program. Think of it like an engine that idles periodically to keep the seals lubricated and the components from seizing up. Without regular blood flow, the smooth muscle in the penile tissue starts to be replaced by fibrotic (scar) tissue. The erections themselves are the maintenance.
In your teens and twenties, you might experience 5-7x erections per night. By your 30s and 40s, that drops to 3-4x. By your 50s and 60s, it's typically 2-3x, with reduced firmness. This decline tracks with the broader changes in vascular health, testosterone levels, and tissue quality that happen with ageing.
The loss of nocturnal erections can be a useful marker of common conditions affecting erectile function — cardiovascular disease, diabetes, hormonal shifts. If you're a bloke who used to wake up reliably at attention and now rarely does, that's not just an inconvenience. It's clinical information.
The Number You Didn't Know You Had
There's a clinical tool called the Erectile Hardness Score. It's a four-point scale that does exactly what the name suggests:

EHS 1 — the penis is larger but not hard.
EHS 2 — hard, but not enough for penetration.
EHS 3 — hard enough for penetration, but not completely hard.
EHS 4 — completely hard and fully rigid.
The EHS was developed in 1998 and is widely used in clinical trials for its simplicity and strong correlation with sexual function outcomes.
Here's what matters: a study of 307 men found that the rate of successful sexual intercourse jumped from 60% at EHS 3 to over 93% at EHS 4. That's a massive gap between "good enough" and "actually good."
A lot of men are sitting at a 3 and calling it normal. Because EHS 3 does work. You can have sex at a 3. It's adequate. But if you were a 4 five years ago and you're a 3 now, you haven't maintained your function — you've lost ground and adjusted your expectations downward. It's like driving a car with a slow tyre leak. You can still steer. But the handling's off, and eventually you're going to notice.
By the time a man reaches his 40s, he has roughly a 40% chance of experiencing some degree of erectile dysfunction, with that figure increasing by about 10% per decade.
Why Your Erection Quality Matters Even When It "Works"
This is where most men check out of the conversation. If it works, why fix it?
Because your erection isn't just a sexual function — it's a barometer. Erectile dysfunction serves as a signal for various underlying conditions, and its significance shouldn't be underestimated just because it doesn't directly threaten life.
But beyond the cardiovascular early-warning system (which we've covered in a previous article), there are specific reasons to actively maintain erectile quality as you age:
Tissue preservation. The ageing process affects the structural organisation of penile erectile tissue, including smooth muscle cells and vascular architecture, leading to reduced elasticity and increased fibrosis. Regular erections — whether spontaneous, stimulated, or assisted — keep oxygenated blood flowing through the cavernosal tissue. Without that regular circulation, the smooth muscle gets progressively replaced by fibrotic tissue. The nightly erections your body produces are already doing this work, but as they decline, you lose the built-in maintenance.
Sensitivity decline. It may take more direct stimulation to achieve an erection with age, and the refractory period between erections increases. Maintaining tissue health helps preserve nerve function longer.
Penile trauma prevention. A penis consistently operating at EHS 3 rather than 4 is structurally less rigid and more vulnerable to buckling injuries during intercourse. These injuries can lead to Peyronie's disease — the development of fibrous plaques that cause curvature and pain. Optimising rigidity isn't vanity; it's structural integrity.
Ejaculatory health. Erectile quality and ejaculatory function are linked. As erection quality declines, so does the force and control of ejaculation with the subsequent refractory period. For men interested in fertility, or simply in maintaining full sexual function, erection optimisation supports the whole system.
The Treatments That Actually Work

PDE5 Inhibitors: The Workhorse
Sildenafil (Viagra), tadalafil (Cialis), and vardenafil (Levitra) remain the first-line treatment. They work by blocking phosphodiesterase type 5, an enzyme that breaks down cGMP — the molecule responsible for relaxing smooth muscle in penile arteries and allowing blood to flow in.
A few things worth knowing. They don't create an erection from nothing — you still need arousal. Tadalafil has a much longer half-life (up to 36 hours versus 4–6 for sildenafil), which is why daily low-dose tadalafil has become popular for maintenance rather than on-demand use. In young men with documented normal function, PDE5 inhibitors primarily reduce the refractory period rather than improving peak rigidity — which suggests that when these drugs produce noticeable improvement, some degree of smooth muscle decline has already begun.
That last point is worth sitting with. If a PDE5 inhibitor makes a meaningful difference to your erection quality, that's useful clinical information — it means the tissue changes of ageing are already underway, and you're catching them at a stage where they're still highly treatable.
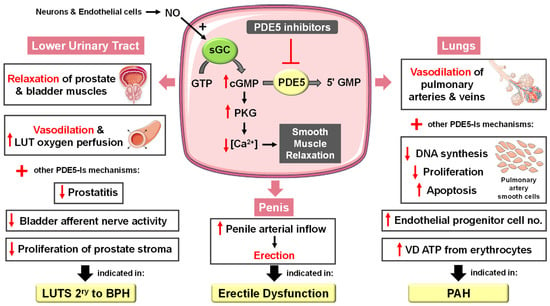
Beyond erections, PDE5 inhibitors have broader vascular benefits. They're approved treatments for pulmonary arterial hypertension, they improve lower urinary tract symptoms associated with BPH, and emerging research suggests roles in cardiovascular protection and cellular ageing. Daily low-dose tadalafil is increasingly viewed as a vascular health intervention, not just an erection pill.
Vacuum Erection Devices: The Underrated Option
If PDE5 inhibitors are the headline act, vacuum erection devices (VEDs) are the roadie who actually makes the show work. Most blokes dismiss them before trying them. That's a mistake.

A VED uses negative pressure to draw blood into the cavernosal tissue, increasing both blood flow and oxygenation. For intercourse, a constriction ring at the base maintains the erection. But for rehabilitation — which is what we're really talking about — the ring often isn't needed. The goal is to flush the tissue with oxygenated blood on a regular basis, essentially supplementing the nightly maintenance your body is doing less effectively as you age.
Studies show that combining a VED for 5 to 10 minutes per day with tadalafil three times weekly achieves success rates of around 90% at one year, compared to 60% with medication alone.
The rehabilitation protocol is straightforward: 3–5 times per week, 5–10 minutes per session, without the constriction ring. Think of it as physio for your penis — consistent, low-intensity maintenance work.
The Pelvic Floor: The Foundation Under Everything
Here's the part most articles skip — and arguably the bit that matters most regardless of what else you're doing.
Your pelvic floor muscles are the structural foundation for erectile function. The bulbocavernosus and ischiocavernosus muscles compress the base of the penis during an erection, trapping blood in the corpora cavernosa and creating the rigidity that takes you from an EHS 3 to an EHS 4. Weak pelvic floor muscles mean less compression, less rigidity, and less ejaculatory control.
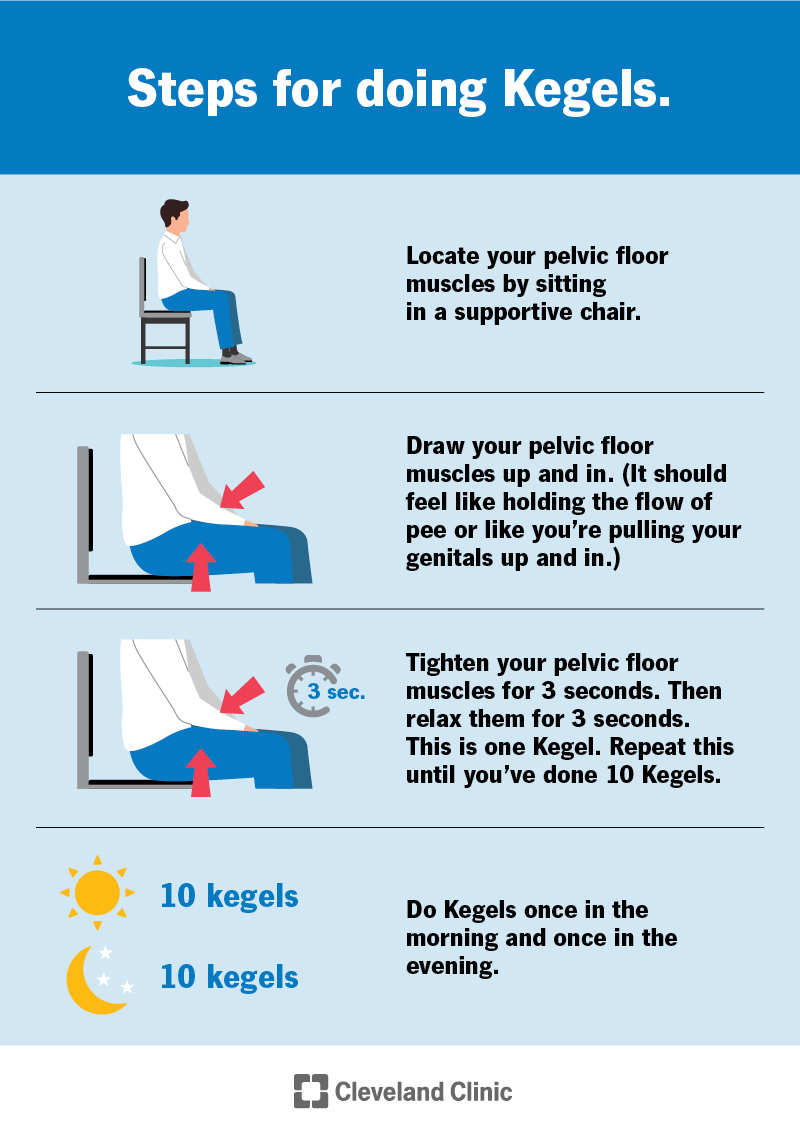
Kegel exercises — the same ones women are told about after childbirth — are the single most underutilised tool in men's sexual health. The exercise itself is simple: contract the muscles you'd use to stop urinating mid-stream, hold for five seconds, release, and repeat. Work up to three sets of ten, daily. If you want to know whether you're engaging the right muscles, try stopping your urine flow once — that's the contraction you're after. Don't make a habit of doing it during urination; that's just the diagnostic.

Core strength more broadly supports the pelvic floor and vascular health that underpin erectile function. A bloke who does regular core work — whether that's yoga, embodiment exercises, pilates, gym-based exercises, or even a proper plank routine — is maintaining the muscular infrastructure that all other treatments build on. No amount of tadalafil compensates for a pelvic floor that's gone to custard. I do have some recommended home based breathwork and core exercises that you may consider as part of your routine here.
This isn't glamorous advice. But it's the stuff that works alongside everything else, costs nothing, has no side effects, and compounds over time.
The Emerging Treatments: What's Showing Promise
Shockwave therapy (Li-ESWT) — a painless, in-clinic treatment delivering low-intensity sound waves to penile tissue — has moved past the "is this real?" phase and into routine use in some practices. The mechanism is stimulation of new blood vessel growth in the tissue. It shows genuine promise for men with mild-to-moderate vascular ED and may offer longer-term restoration of natural function.

Radiofrequency therapy is the newer entrant worth watching. The Vertica device uses low-intensity radiofrequency energy, applied via a handheld home-use device, to gently warm penile tissue. The rationale is that RF energy can restore the structural arrangement of collagen fibres in the tunica albuginea — the sheath around the erectile tissue that acts as the hydraulic seal during an erection. An ongoing pivotal clinical trial is assessing the device against sham treatment in men with mild-to-moderate ED, and a pilot study of 28 men showed significant improvements in both IIEF and Erection Hardness Scores, with half of participants achieving normal erectile function parameters. UCI Health in the US has opened the first American clinical trial of the device. It's early days, but the concept — a drug-free, home-use device that targets the collagen integrity of the erectile mechanism — is genuinely interesting.
PRP (Platelet-Rich Plasma) involves drawing your own blood, concentrating the platelets (which are rich in growth factors), and injecting the resulting plasma into the penile tissue. The theory is that those growth factors promote tissue repair, blood vessel regeneration, and potentially improved nerve function. There is increasing interest in PRP as a regenerative therapy that may address the underlying causes of ED rather than just managing symptoms. However, there is still no conclusive evidence regarding its efficacy — early randomised trials show promise, but scientific bodies including the American Urological Association have stated that PRP should only be used for ED in the context of clinical trials. It's not snake oil, but it's not proven either.
The Rest of the Toolkit
Lifestyle modification remains the foundation. Exercise, weight management, smoking cessation, and alcohol moderation all directly improve vascular function. If you're carrying an extra 15 kilos around the middle, no medication will fully compensate for the vascular damage that causes.
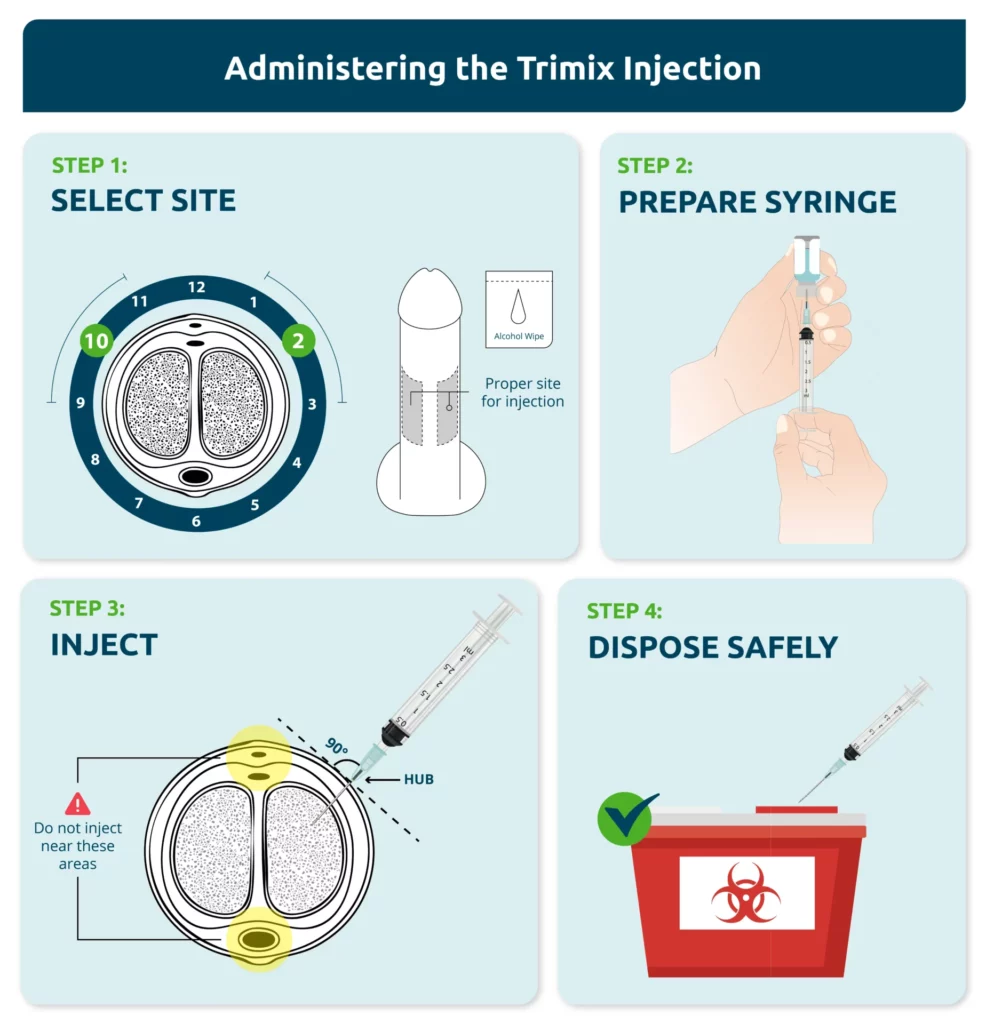
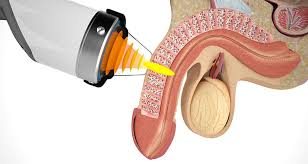
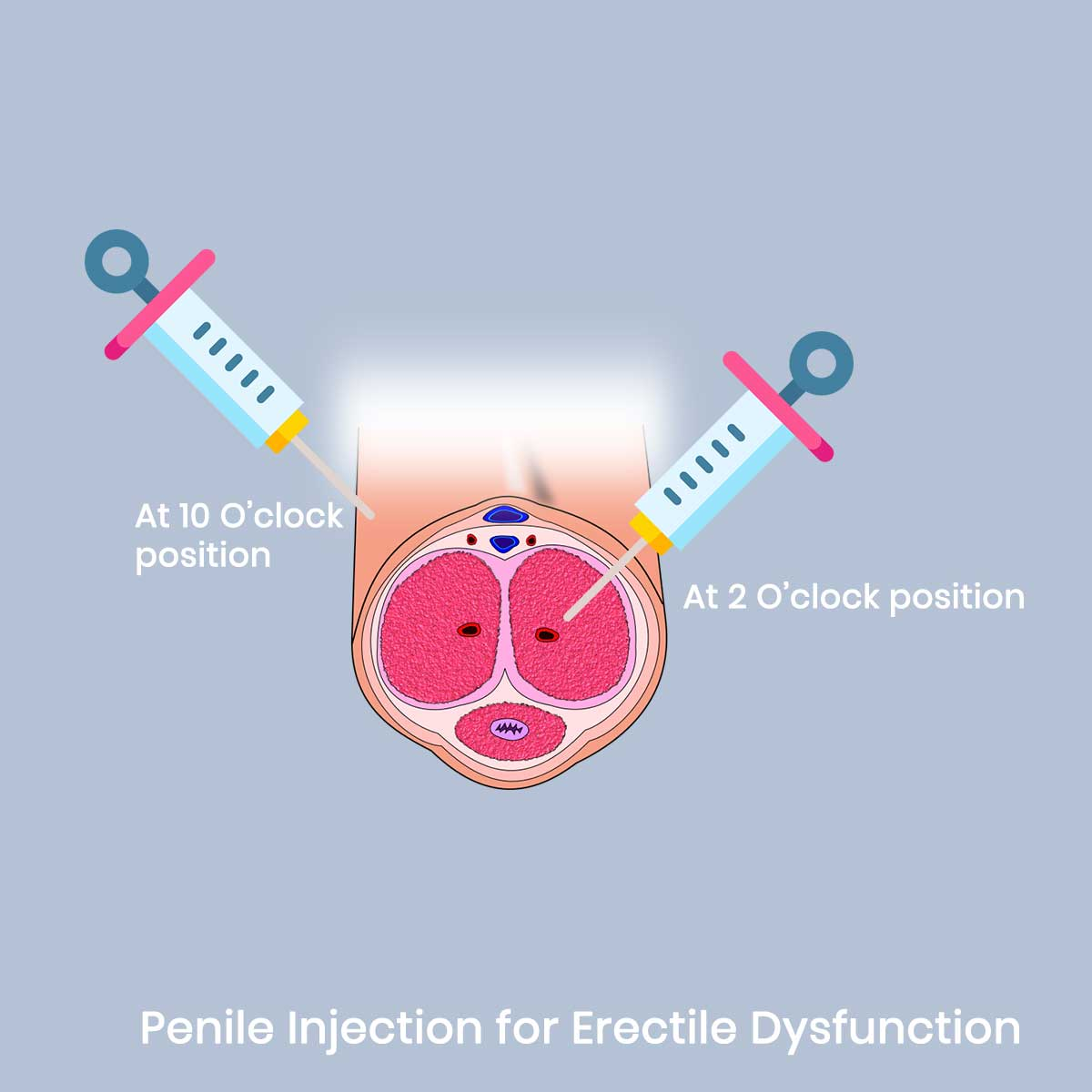
Intracavernosal injections (Trimix or alprostadil) are an option when oral medications aren't sufficient — highly effective but require injecting into the base of the penis before intercourse.
Penile implants remain the last resort for men who've exhausted other options. Satisfaction rates are high, but it's irreversible.

The Preventive Case
Here's the reframe that matters most: you don't need to have a problem to benefit from optimising your erectile health. If you're over 40, your penile tissue is already changing. Ageing brings smooth muscle cell loss, fibrotic remodelling, reduced nitric oxide production, and declining nerve function.
Your body's own overnight erections — the original maintenance program — are declining in frequency and quality. The question isn't whether to replace that lost maintenance. It's how.
Daily low-dose tadalafil plus regular VED use is increasingly prescribed not as a treatment for ED, but as a prevention strategy. Layer consistent pelvic floor work and core strength underneath that, and you have a comprehensive maintenance program that addresses tissue health, vascular function, and the muscular infrastructure all at once.
The men who maintain strong function into their 60s and 70s aren't lucky — they're the ones whose vascular health, hormonal environment, tissue integrity, and pelvic floor strength have been maintained, whether by genetics, lifestyle, or deliberate intervention.


