
Here’s what happens to them — and why it matters after a vasectomy.
It starts with a stem cell
Every sperm cell begins its life deep inside the testicle, in tightly coiled tubes called seminiferous tubules. If you unwound all of them from a single testicle, they’d stretch about 250 metres — roughly the length of two and a half rugby fields.
Lining the walls of these tubules are spermatogonial stem cells — the “mother cells” of the sperm production line. Unlike most stem cells in your body, these never stop dividing. From puberty until the day you die, they’re continuously producing new generations of sperm. There’s no retirement age for your testicles.
The process of turning a stem cell into a mature sperm is called spermatogenesis, and it takes approximately 74 days — just under 11 weeks. That means the sperm in today’s ejaculation were “born” back when you were doing whatever you were doing two and a half months ago.
|
⚡ Fun fact Your testicles produce roughly 1,500 sperm
per second — that’s about 130 million per day, or around 40–50 billion
per year. In a lifetime, a man produces approximately 500 billion sperm. Only
a tiny handful will ever fertilise an egg. |
Why your testicles hang outside your body
Spermatogenesis is remarkably temperature-sensitive. It requires a temperature about 2–4°C cooler than core body temperature — which is why the testicles sit outside the body in the scrotum. Your body has an elegant thermostat for this: the cremaster muscle raises the testicles closer to the body when it’s cold and lowers them when it’s warm. The pampiniform venous plexus — a network of veins wrapped around the testicular artery — acts as a countercurrent heat exchanger, cooling arterial blood before it reaches the testicle. It’s the same engineering principle used in industrial cooling systems.
This is also why prolonged heat exposure (hot tubs, saunas, laptops on laps, tight underwear) can temporarily reduce sperm production — you’re overriding the thermostat.
|
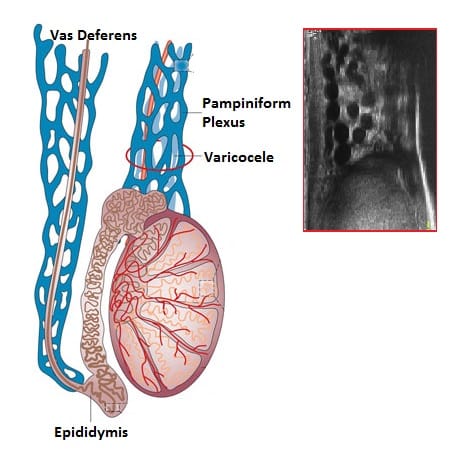
⚡ Fun fact A varicocele — an enlargement of the
veins in the scrotum — is the most common correctable cause of male
infertility. It works by disrupting that heat exchange system, effectively
warming the testicle and impairing sperm production. |
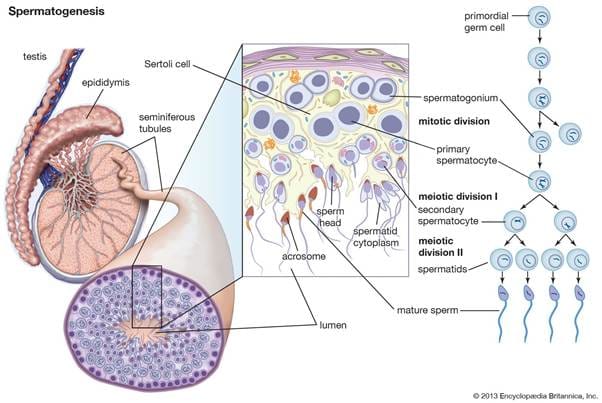
The 74-day journey: from round cell to racing tadpole
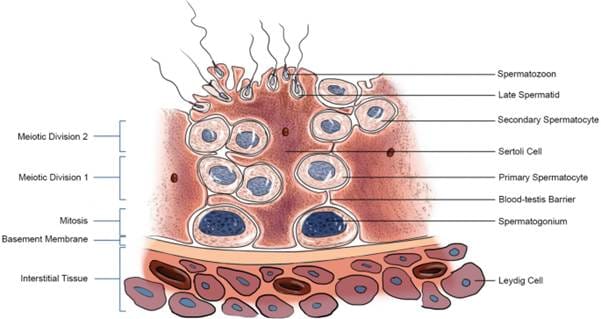
Spermatogenesis unfolds in stages, each with increasingly specialised cells. It begins with the spermatogonial stem cell dividing by mitosis to produce spermatocytes. These undergo meiosis — the special cell division that halves the chromosome number from 46 to 23 — creating spermatids. Each original cell eventually produces four spermatids, each carrying either an X or a Y chromosome. This is the moment that determines the sex of any future child.
The spermatids then undergo a dramatic transformation called spermiogenesis. The round cell reshapes itself into the streamlined sperm we’d recognise under a microscope: a compact head packed with DNA, a midpiece loaded with mitochondria (the energy generators), and a long tail (flagellum) for propulsion. The cell sheds most of its cytoplasm — it’s essentially stripping down to the bare essentials for one purpose: delivering DNA to an egg.
Throughout this process, Sertoli cells — sometimes called “nurse cells” — physically cradle the developing sperm, feeding them nutrients, removing waste, and forming a barrier (the blood-testis barrier) that shields them from the immune system. This barrier is critical — without it, your immune system would recognise sperm as foreign and attack them. (More on this later, because it becomes directly relevant after vasectomy.)
|
⚡ Fun fact Sperm are among the smallest cells in
the human body, while the egg they’re trying to reach is the largest.
A single egg is about 85,000 times the volume of a single sperm. |
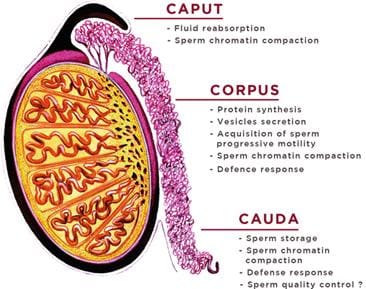
Finishing school: the epididymis
When sperm leave the seminiferous tubules, they look like mature sperm but can’t actually do anything useful — they can’t swim effectively and can’t fertilise an egg. They need to spend another 2–3 weeks maturing in the epididymis, a tightly coiled tube sitting on top of each testicle.
The epididymis is divided into three sections: the head (caput), body (corpus), and tail (cauda). As sperm travel through, they undergo a series of biochemical changes to their cell membrane — a process called epididymal maturation. They acquire the ability to swim in a directed, progressive pattern rather than just twitching in circles. They also gain surface proteins that will later be essential for recognising and binding to an egg.
The tail of the epididymis (cauda) is the main storage depot for mature, ready-to-go sperm. Sperm can survive here for several weeks. If they’re not ejaculated, they eventually age, die, and are reabsorbed by the body. This is normal — your body has been recycling unused sperm your entire adult life.
From the epididymis, sperm enter the vas deferens — the tube that is cut and sealed during a vasectomy.
The final sprint: ejaculation
When ejaculation occurs, sperm are rapidly propelled from the epididymis through the vas deferens to the ampulla near the prostate, then through the ejaculatory duct into the urethra. They’re mixed with fluids from the seminal vesicles (which provide fructose as fuel and make up about two-thirds of the semen volume) and the prostate (which adds enzymes and zinc). This mixed fluid is then expelled in a series of approximately eight pulsatile jets driven by rhythmic contractions of the pelvic floor muscles.
At this point, sperm are swimming but are still not capable of fertilising an egg. One final transformation remains.
Capacitation: the activation switch
After ejaculation — assuming no vasectomy — sperm that reach the female reproductive tract undergo a process called capacitation. This takes several hours and is triggered by the chemical environment inside the uterus and fallopian tubes.
During capacitation, cholesterol is stripped from the sperm’s outer membrane, making it more fluid and unstable. Calcium floods into the cell. The swimming pattern changes from steady forward motion to a hyperactivated, whip-like thrashing that generates the force needed to push through the layers surrounding the egg. Think of it as switching from cruising gear to full throttle.
Only capacitated sperm can perform the acrosome reaction — the final act.
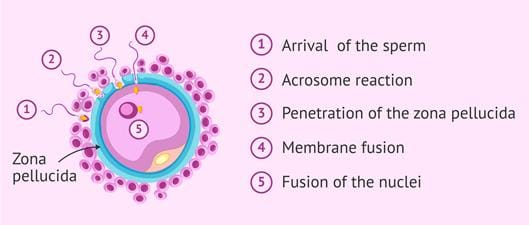
The acrosome reaction: the grand finale
The acrosome is a cap-like structure covering the front of the sperm head, packed with digestive enzymes. When a capacitated sperm contacts the zona pellucida (the tough outer shell of the egg), the acrosome ruptures, releasing these enzymes. They dissolve a path through the zona, allowing the sperm to reach and fuse with the egg’s cell membrane.
The moment one sperm fuses with the egg, the zona pellucida undergoes a rapid chemical change — called the cortical reaction — that locks out all other sperm. Out of the hundreds of millions of sperm in a single ejaculate, only a few hundred reach the egg, and only one gets in.
|
⚡ Fun fact The journey from vagina to egg is, relative
to the sperm’s size, the equivalent of a human swimming from New Zealand
to Australia. The vast majority don’t make it — the female reproductive
tract is essentially an obstacle course designed to select only the most
capable sperm. |
So after a vasectomy — where do they all go?
Your vasectomy cuts and seals the vas deferens, blocking sperm from reaching the ampulla and the ejaculate. But your testicles don’t get the memo — they keep producing sperm at exactly the same rate. So what happens to 130 million sperm a day with nowhere to go?
Most are simply reabsorbed
This is actually the same thing that happened before your vasectomy — the majority of sperm produced were never ejaculated, aged and quietly broken down and recycled in the epididymis by principal and clear cells at the lining of the epididymis. After vasectomy, the proportion being reabsorbed simply increases to 100%. The epididymal lining contains specialised cells that break down and absorb ageing sperm. This is a normal, painless, ongoing process.
Pressure may build — briefly
In the weeks after vasectomy, there can be a transient increase in pressure in the epididymis as the system adjusts to the blocked outflow. The reabsorption system becomes activated and the epididymis adapts and may becomes dilated to match the higher load. Some sperm may leak out from the epithelium or from the cut part of the vas deferens (causing sperm granuloma).
For most men, this causes no symptoms at all. In some men, this adjustment period can cause a dull ache or fullness in the testicle that usually settles within a few weeks.
Sperm granulomas can form
Occasionally, sperm leak from the cut end of the vas or from the epididymis. When sperm escape into the surrounding tissue, your immune system — which normally never encounters sperm because of the blood-testis barrier — recognises them as foreign and mounts an inflammatory response. The result is a small nodule called a sperm granuloma, usually at the vasectomy site. Most granulomas are tiny, painless, and never noticed. In fact, some surgeons deliberately leave the testicular end of the vas open (open-ended vasectomy) to allow controlled sperm leakage, which may reduce epididymal pressure and lower the risk of post-vasectomy discomfort.
Anti-sperm antibody may or may not develop
Through this whole process, the blood-epididymis barrier (formed by tight junctions between those principal cells of the epididymis) keeps all of this contained away from blood vessels to keep the sperm antigens separate from blood vessels. Therefore the immune system stays ignorant, and reabsorption happens quietly without triggering autoimmunity. It's only when that barrier is breached (trauma, surgery, granuloma) that anti-sperm antibodies can develop.
Production may slow slightly over time
Some long-term studies suggest that sperm production rate decreases modestly years after vasectomy, likely because of chronic back-pressure effects on the seminiferous tubules. This is one reason why vasectomy reversal success rates decline with time — not just because of scarring at the vasectomy site, but because the factory itself may have slowed down.
|
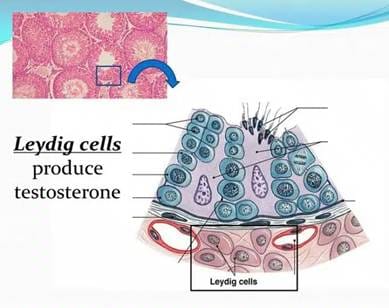
⚡ Fun fact Despite all of this, vasectomy has no
effect on testosterone levels. Testosterone is produced by Leydig cells
in the testicle and enters the bloodstream directly — it never travels
through the vas deferens. Your hormones, libido, erections, and ejaculate
volume are all unaffected. |
What if I change my mind? Fertility after vasectomy
A vasectomy is intended to be permanent — but life doesn’t always go to plan. About 3–6% of men who’ve had a vasectomy eventually explore having another child. If that’s you, it’s worth understanding your options, because the biology of sperm we’ve just covered directly affects your chances.
Your testicles are still making sperm. As we’ve discussed, a vasectomy doesn’t switch off the factory. Sperm production continues, and for most men the machinery stays functional for years. That said, there’s evidence that long-term back-pressure on the epididymis and seminiferous tubules can gradually reduce sperm production quality over time. This is one reason why the duration since your vasectomy matters — not just because of scarring at the vasectomy site, but because the sperm-producing system itself may have changed.
Option 1: Vasectomy reversal (microsurgical reconstruction)
This involves reconnecting the cut ends of the vas deferens under a surgical microscope. Current guidelines from both the European Association of Urology (2025) and the American Urological Association (2026) recognise microsurgical vasectomy reversal as a viable first-line option, with patency rates of 90–97% (sperm returning to the ejaculate) when performed by experienced microsurgeons. However, patency doesn’t guarantee pregnancy — actual pregnancy rates are lower and depend heavily on several factors.
The three strongest predictors of success after reversal are how long ago the vasectomy was done (shorter intervals = better outcomes), the man’s age, and the female partner’s age. If the surgeon finds thick, paste-like fluid with no sperm at the vasectomy site during the operation, it may indicate a secondary blockage further back in the epididymis, which requires a more complex repair called a vasoepididymostomy. This is why guidelines recommend that any surgeon offering vasectomy reversal should also have the microsurgical expertise to perform this more advanced procedure if needed.
One important tip from recent guidelines: if a reversal is initially successful and sperm return to the ejaculate, it’s worth freezing a semen sample as backup. In about 10% of men, the reconnection can scar closed again over time (delayed anastomotic fibrosis), so having frozen sperm available provides insurance.
Option 2: Surgical sperm retrieval + IVF/ICSI
Instead of rebuilding the pipeline, sperm can be extracted directly from the epididymis or testicle and used for in vitro fertilisation with intracytoplasmic sperm injection (ICSI) — where a single sperm is injected directly into an egg.
For post-vasectomy men, sperm can be retrieved from the epididymis (where mature sperm are stored) using either a simple needle aspiration through the skin called percutaneous epididymal sperm aspiration (PESA) or a more precise microsurgical technique called microsurgical epididymal sperm aspiration (MESA) done through a small incision and epididymal tubule magnification that typically yields more sperm which can be frozen for future use. Alternatively, a small biopsy can be taken directly from the testicle called testicular sperm extraction (TESE) or microdissection TESE done with a high powered operating microscope for better sampling precision (usually reserved for non-vasectomy causes). Because sperm production is completely normal after vasectomy — the problem is just a blockage — retrieval is almost always successful regardless of the technique used.

Pregnancy outcomes with ICSI are comparable whether sperm comes from the epididymis or testicle, and whether it's used fresh or frozen. Because ICSI only needs a single sperm per egg, even small numbers of retrieved sperm are sufficient. Any surplus can be frozen for future cycles, potentially avoiding the need for a second retrieval.
Which option is better?
There’s no single right answer — guidelines from the AUA, EAU, and the recently published first Australian male infertility guidelines (2025) all emphasise that this should be a shared decision between the couple and their doctors, based on individual circumstances. Key considerations include:
• The female partner’s age and fertility status — this is often the most important variable
• The time since vasectomy — longer intervals reduce reversal success rates
• Cost and accessibility — reversal is typically less expensive than IVF but isn’t always funded
• Whether you might want more than one child — reversal restores natural fertility, meaning multiple pregnancies are possible without further procedures
• Your comfort with the IVF process
Some couples choose both — having a reversal performed while simultaneously retrieving and freezing sperm, so that if the reversal doesn’t work, IVF can proceed without a second surgical procedure.
What about men who haven’t had a vasectomy but are struggling with fertility?
Understanding sperm biology is just as relevant if you’re trying to conceive and things aren’t happening. Current international guidelines recommend that any man in a couple experiencing infertility should have a proper assessment — including a detailed history, physical examination, and semen analysis — rather than jumping straight to assisted reproduction. In about half of infertile couples, a male factor is involved, and some of these are specifically treatable.
Importantly, recent guidelines also highlight that men with abnormal semen parameters should be counselled about their broader health. Male infertility is increasingly recognised as a window into overall health — infertile men have higher rates of cardiovascular disease, metabolic conditions, and even certain cancers compared to fertile men. A fertility assessment isn’t just about making a baby — it can be an early warning system for your long-term health.
If you have concerns about your fertility — whether before or after a vasectomy — talk to your GP or a reproductive medicine specialist. Early assessment gives you the best range of options.
|
The bottom line Sperm are
extraordinary cells — purpose-built, ruthlessly streamlined, and produced in
staggering numbers. After a vasectomy, the production line keeps running, but
your body has well-established systems for recycling what it no longer needs.
Understanding this biology helps explain why a vasectomy doesn’t change how
you feel, why it takes time to clear residual sperm, and why the occasional
post-vasectomy ache is usually just your body adjusting to the new plumbing
arrangements. |


