
Erectile dysfunction isn’t a bedroom problem. It’s a cardiovascular warning sign that shows up years before a heart attack — if you know how to read it.
This is a series of two articles Part 1 "Why your Erection is a Window Into Your Heart?" and Part II "How to improve erections?".
The Conversation No One Wants to Have
Let’s be honest. If a bloke in his 40s notices things aren’t working as reliably in the bedroom, his first instinct isn’t to book in with his GP. He’ll blame stress. He’ll blame the beers. He’ll quietly open an incognito browser tab at midnight and try to convince himself it’s nothing.
That’s completely understandable. Erectile dysfunction (ED) sits right at the intersection of masculinity, vulnerability, and shame — three things most men would rather not examine simultaneously.
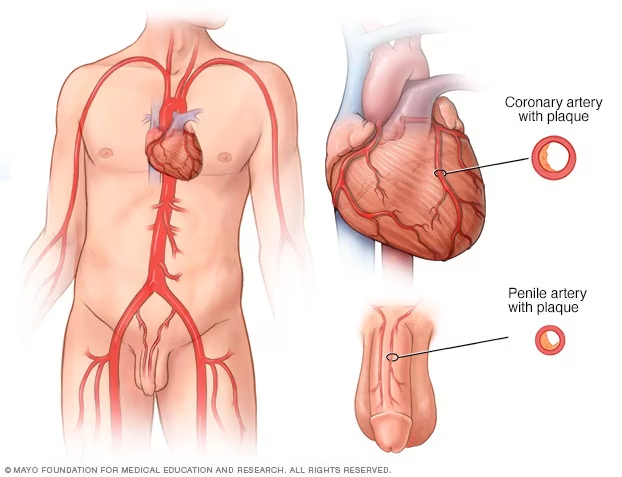
But here’s what I need you to hear, because it might genuinely save your life: your erection is one of the most sensitive early warning systems your body has. It’s not just about sex. It’s about blood flow. And the same process that’s quietly reducing blood flow to your penis is doing exactly the same thing to your coronary arteries — the ones feeding your heart.
The difference? Your penile arteries are about 1–2mm in diameter. Your coronary arteries are 3–4mm. The small pipes clog first. That’s not a metaphor. It’s plumbing.
Small Pipes, Big Warning
In 2003, an Italian cardiologist named Piero Montorsi published a landmark study that shifted the way medicine thinks about erections. He found that in men who’d had a heart attack, nearly two-thirds had experienced erectile dysfunction beforehand — and on average, ED had appeared three years before the cardiac event.
Three years. That’s not a coincidence. That’s a lead time.
The explanation is elegant and intuitive: atherosclerosis — the gradual build-up of fatty plaque inside artery walls — is a systemic disease. It doesn’t target one artery in isolation. It’s happening everywhere. But you’ll notice it first wherever the arteries are smallest, because even a small amount of plaque in a tiny artery causes a proportionally larger reduction in blood flow.
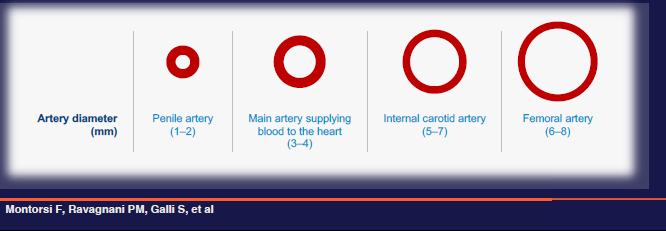
Think of it like this. Imagine the same thin layer of grime building up on the inside of a garden hose and the inside of a stormwater drain. The drain barely notices. The garden hose? Flow drops off a cliff. Your penile arteries are the garden hose.
This is sometimes called the “artery size hypothesis,” and it’s now well-established in cardiovascular medicine. ED in a man under 55 with no other obvious cause should be treated as a vascular red flag until proven otherwise.
The Invisible Process Behind Both Problems
To understand why erections and heart health are connected, you need to understand one concept: endothelial function.
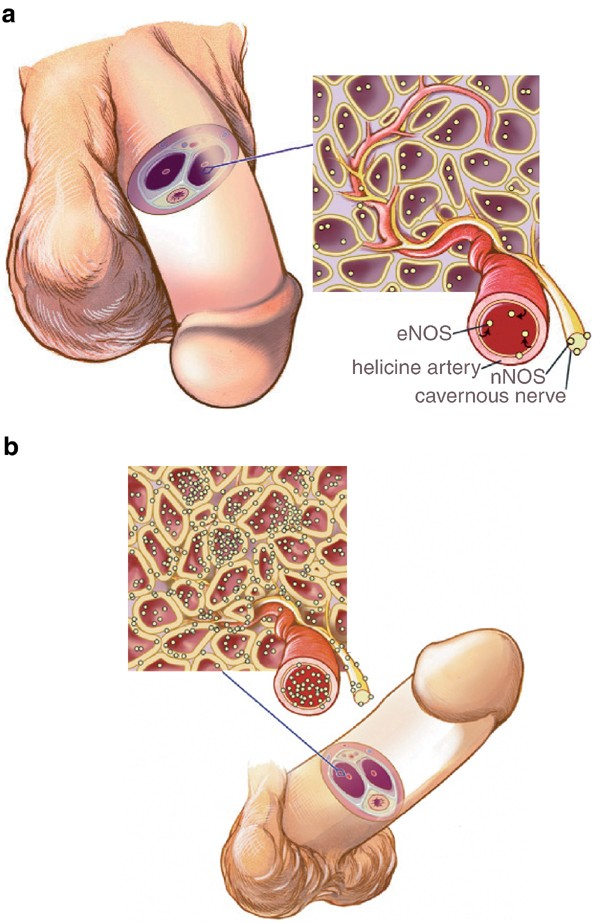
The endothelium is a single-cell-thick lining inside every blood vessel in your body. When it’s healthy, it produces nitric oxide — a gas that tells the smooth muscle surrounding the artery to relax, allowing the vessel to dilate and blood to flow freely. This is the fundamental mechanism behind an erection: nitric oxide release triggers arterial dilation in the penis, which allows rapid inflow of blood into the erectile tissue.
It’s also the mechanism that keeps your coronary arteries responsive and flexible.
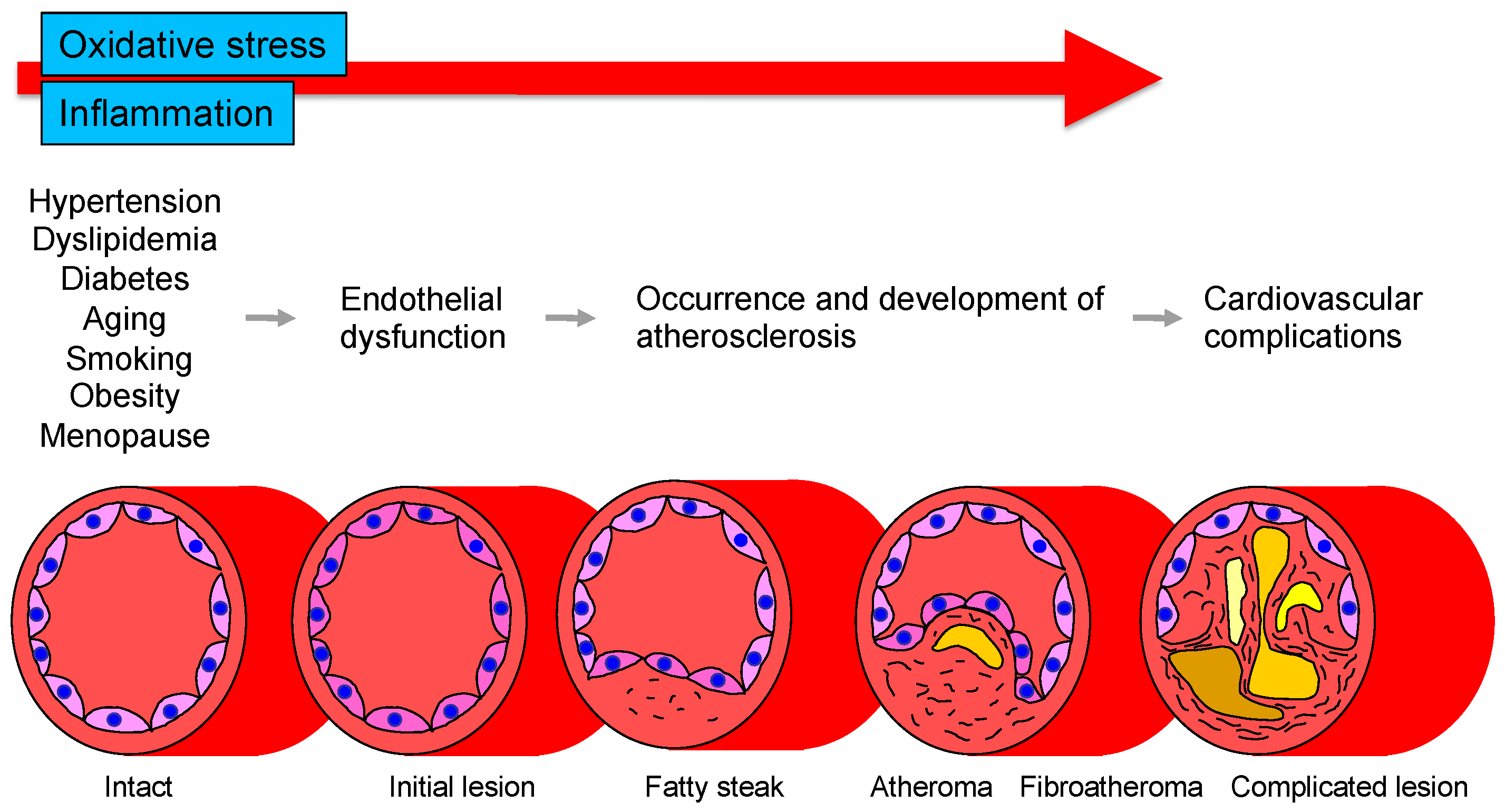
When the endothelium becomes damaged — by high blood pressure, elevated blood sugars, smoking, chronic inflammation, or poor metabolic health — nitric oxide production drops. Arteries become stiffer, less responsive, and more vulnerable to plaque formation. This is endothelial dysfunction, and it’s the earliest detectable stage of cardiovascular disease. It shows up before any plaque is visible on a scan, before any cholesterol number looks alarming, and long before a heart attack.
And where does it show up first? You already know the answer.
It’s More Than Plumbing
The artery size hypothesis is a useful framework, but the connection between ED and cardiovascular disease goes deeper than just narrowed pipes. They share an overlapping web of risk factors that tend to travel together:
Insulin resistance and metabolic syndrome. Elevated blood sugars damage the endothelium directly. Insulin resistance also drives up inflammation and reduces nitric oxide bioavailability. Men with metabolic syndrome have roughly double the risk of ED compared to metabolically healthy men.
Visceral adiposity. Excess fat stored around the organs — particularly abdominal fat — is metabolically active tissue that pumps out inflammatory cytokines and converts testosterone to oestrogen via aromatisation. The result: lower testosterone, higher inflammation, and impaired vascular function. All three contribute independently to both ED and cardiovascular risk.
Hypertension. High blood pressure damages the endothelium over time, and many antihypertensive medications (particularly older beta-blockers and thiazide diuretics) can worsen erectile function. It’s a double hit.
Dyslipidaemia. Elevated LDL cholesterol and triglycerides accelerate plaque formation. Oxidised LDL is directly toxic to endothelial cells.
Smoking and sedentary behaviour. Both are potent drivers of endothelial dysfunction. Smoking damages the vascular lining with every cigarette. A sedentary lifestyle reduces the shear stress on vessel walls that normally stimulates nitric oxide production.
When a man presents with ED, he’s often not dealing with one of these factors in isolation. He’s dealing with three or four simultaneously. That clustering is what makes ED such a powerful early signal — it’s not flagging a single risk factor, it’s flagging a metabolic pattern.
What the Evidence Actually Shows
The data on ED as a cardiovascular predictor is now substantial enough that major cardiology guidelines have incorporated it. The European Society of Cardiology includes ED as a risk factor in its cardiovascular risk assessment frameworks. The Princeton Consensus guidelines specifically recommend cardiac evaluation for men presenting with ED.
The Thompson data from the Prostate Cancer Prevention Trial — one of the largest datasets we have — found that men who developed ED during the study had a 25% increase in subsequent cardiovascular events, even after adjusting for traditional risk factors. That tells us something important: ED isn’t just a marker for the risk factors we already know about. It appears to carry independent predictive value, likely because it’s capturing subclinical vascular damage that standard blood tests miss.
A meta-analysis published in the Journal of the American College of Cardiology found that men with ED had a 44% higher risk of cardiovascular events, a 62% higher risk of heart attack, and a 39% higher risk of stroke compared to men without ED. These are not trivial numbers.
What a Proper Workup Looks Like
If you’re a man between 35 and 55 and you’re experiencing erectile difficulties, here’s what a thorough assessment should include — and it goes well beyond a script for sildenafil:
Metabolic bloodwork. Fasting glucose and insulin (not just HbA1c alone), a comprehensive lipid panel, liver function, and inflammatory markers like hsCRP. The goal is to detect insulin resistance and metabolic dysfunction early, before diabetes is diagnosed.
Hormonal assessment. Total testosterone, SHBG, and a calculated free testosterone. Low testosterone is both a cause of ED and an independent cardiovascular risk marker. It’s also commonly missed when GPs only check total testosterone without considering SHBG, which can mask a low free testosterone behind a “normal” total number.
Cardiovascular risk assessment. Blood pressure, waist circumference, family history, and ideally a coronary artery calcium (CAC) score for men whose risk profile warrants it. A CAC score is a low-radiation CT scan that directly measures calcified plaque in your coronary arteries — it’s the single best tool we have for reclassifying a man from “probably fine” to “needs attention.”
Lifestyle and psychological screen. Sleep quality (obstructive sleep apnoea is massively underdiagnosed and independently worsens both ED and cardiovascular risk), alcohol intake, exercise patterns, and mental health. Depression, anxiety, and relationship stress can all drive ED through neurological and hormonal pathways, but they can also coexist with genuine vascular disease. Both need to be addressed.
The point is that a man presenting with ED deserves a comprehensive health assessment, not a rushed prescription. The erection problem is the tip of the iceberg. The job of a good clinician is to look at what’s underneath.
What You Can Actually Do About It
The encouraging news is that the same interventions that improve cardiovascular health tend to improve erectile function, often significantly. This isn’t about choosing between your heart and your sex life — they’re the same project.
Exercise is the single most effective intervention. Aerobic exercise directly improves endothelial function and nitric oxide production. Resistance training supports testosterone levels and metabolic health. A meta-analysis of lifestyle interventions for ED found that exercise alone produced improvements comparable to PDE5 inhibitors (drugs like Viagra and Cialis) in men with mild to moderate ED. You don’t need to become a marathon runner. Consistent moderate-intensity activity — 150 minutes per week — makes a measurable difference.
Body composition matters more than body weight. Losing visceral fat reduces inflammation, improves insulin sensitivity, increases testosterone, and directly improves vascular function. Even modest fat loss — 5 to 10 percent of body weight — can meaningfully improve erectile function in overweight men.
Dietary patterns over dietary rules. Mediterranean-style eating patterns consistently show the strongest evidence for both cardiovascular protection and improved erectile function. The common thread is likely the anti-inflammatory and endothelial-protective effects of polyphenols, omega-3 fatty acids, and fibre. You don’t need to be perfect. You need to be consistent.
Quit smoking. The endothelial damage from smoking is dose-dependent and partially reversible. Men who quit show measurable improvements in vascular function within weeks.
Optimise sleep. Poor sleep — particularly untreated obstructive sleep apnoea — drives sympathetic nervous system activation, raises blood pressure, worsens insulin resistance, and suppresses testosterone. Fixing sleep is one of the highest-yield interventions available and one of the most overlooked.
Medications when indicated. PDE5 inhibitors are not just a band-aid. There’s emerging evidence that regular use may have direct endothelial-protective effects, and they can serve as a valuable bridge while lifestyle changes take hold. Statins, antihypertensives (particularly ACE inhibitors and ARBs, which are erectile-friendly), and metformin for insulin resistance all address the underlying vascular pathology. And for men with genuinely low testosterone, appropriately managed testosterone therapy can improve both erectile function and cardiovascular risk markers simultaneously.

The Conversation Worth Having
Here’s what I want you to take away from this.
If you’re experiencing erectile difficulties, you haven’t “failed” at anything. Your body is doing you a favour. It’s giving you a signal — a measurable, evidence-based, clinically validated signal — that something in your vascular system needs attention. And it’s giving you that signal years before the consequences become irreversible.
That’s not bad news. That’s an opportunity most men never get. Heart attacks don’t usually send a warning letter. But in this case, your body is sending one. The question is whether you’ll read it.
The men who do best are the ones who reframe the conversation. ED isn’t a shameful secret to manage with a discreetly ordered pill. It’s a clinical finding that opens the door to a proper assessment of your metabolic, hormonal, and cardiovascular health — the kind of assessment that can genuinely change your trajectory.
Talk to your GP. Get the bloodwork done. Ask about your vascular health. And if your GP hands you a script for sildenafil without checking your fasting insulin, your testosterone, your blood pressure, and your waist circumference — find one who will.
Your erection is trying to tell you something. It’s worth listening.
If you are interested to explore more, please read Part II of our series, how do I get stronger erections?.
Key References
Montorsi F, et al. Association between erectile dysfunction and coronary artery disease: a case report study. J Urol. 2003;170(4 Pt 1):1256–1259.
Thompson IM, et al. Erectile dysfunction and subsequent cardiovascular disease. JAMA. 2005;294(23):2996–3002.
Dong JY, et al. Erectile dysfunction and risk of cardiovascular disease: meta-analysis of prospective cohort studies. J Am Coll Cardiol. 2011;58(13):1378–1385.
Vlachopoulos CV, et al. Prediction of cardiovascular events and all-cause mortality with erectile dysfunction: a systematic review and meta-analysis of cohort studies. Circ Cardiovasc Qual Outcomes. 2013;6(1):99–109.
Nehra A, et al. The Princeton III Consensus recommendations for the management of erectile dysfunction and cardiovascular disease. Mayo Clin Proc. 2012;87(8):766–778.
Esposito K, et al. Effect of lifestyle changes on erectile dysfunction in obese men: a randomized controlled trial. JAMA. 2004;291(24):2978–2984.