
Prostate cancer is now the most commonly diagnosed cancer in Australia — and it's hitting younger men harder than ever. Here's what's changed, what to ask your GP, and why most of what you've heard about testosterone and prostate cancer is wrong.
Let's start with the number that should get your attention. The rate of prostate cancer among Australian men aged 40–49 has surged from 4.9 cases per 100,000 in 2000 to 12.5 in 2025 — an increase of more than 150%. Deaths in men under 50 have risen 200% since 2014. There's also been a 500% increase in rates of men aged 30–39 being diagnosed.
In 2025, an estimated 28,868 Australian men will be diagnosed with prostate cancer — roughly 79 men every day. One in five will be diagnosed in their lifetime. And nearly 4,000 will die from it this year — over 11 men a day.
This is not a disease that waits until you're 70. And the screening landscape has fundamentally changed.
What Screening Actually Looks Like Now
If your last prostate conversation with your GP was five years ago, the guidance has moved on significantly.
The PSA blood test remains the front door. Current Australian NHMRC-endorsed guidelines recommend that well-informed men aged 50–69 have PSA screening every two years, with further investigation if the total PSA is above 3.0 ng/mL. Earlier screening — from age 40 — is recommended for men with a family history of prostate cancer or of sub-Saharan African ancestry.

But here's the big shift: under the draft 2025 guidelines, biopsy is no longer the primary test after an elevated PSA. Multiparametric MRI (mpMRI) is now the preferred first diagnostic test, and the MRI determines whether a biopsy is needed at all.
This is a game-changer. The old pathway — elevated PSA, straight to a transrectal biopsy — was painful, carried infection risk, and frequently detected cancers that were clinically insignificant. mpMRI-targeted biopsy has a sensitivity of 87% for clinically significant prostate cancer compared to 60% for the old ultrasound-guided approach. It finds the cancers that matter and avoids the ones that don't.
Australia is a global pioneer in using mpMRI and PSMA PET/CT for prostate diagnostics, benefiting from government-based Medicare rebates that have improved access even in regional areas. If your GP isn't using this pathway, ask why.
BPH and LUTS: The Stuff That Isn't Cancer But Still Ruins Your Life
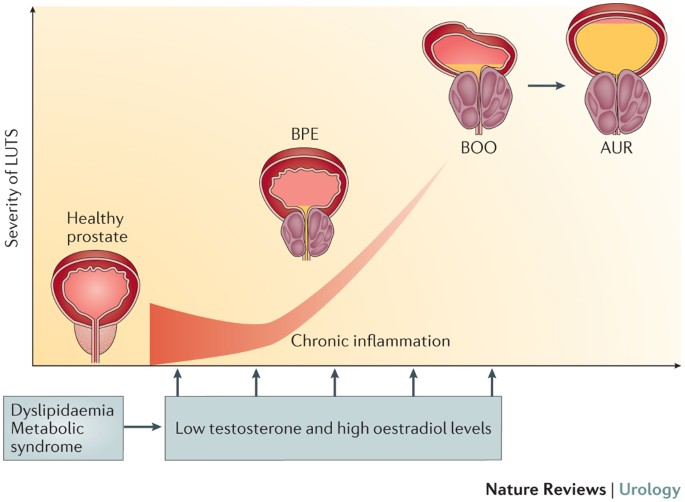
Not everything prostate-related is cancer. Benign prostatic hyperplasia (BPH) — non-cancerous enlargement of the prostate — affects roughly half of men by age 50 and up to 90% by age 80. The symptoms are collectively called lower urinary tract symptoms (LUTS): getting up multiple times at night to pee, weak stream, urgency, the feeling you haven't fully emptied, and the slow dribble that makes you linger at the urinal longer than you'd like.
Most blokes write this off as ageing. It's not. It's a treatable condition, and ignoring it affects sleep quality, daily function, and — less obviously — sexual health.
This is where PDE5 inhibitors re-enter the picture. Daily low-dose tadalafil (Cialis) is now a recognised treatment for LUTS associated with BPH — not just for erectile dysfunction. The mechanism is smooth muscle relaxation in the prostate, bladder neck, and urethra, which reduces resistance to urine flow. It simultaneously improves blood flow to penile tissue, maintaining the smooth muscle health that prevents the fibrotic changes underlying erectile dysfunction.
Think of daily tadalafil as serving double duty: it addresses the urinary symptoms of an ageing prostate and preserves the penile tissue health that keeps your erectile function intact. For a man in his 40s or 50s with early LUTS and early erectile changes, it's one medication treating two interconnected problems through the same vascular mechanism.
Does Regular Ejaculation Help Prevent Prostate Cancer?
This is the section every bloke reads twice. The largest and strongest study on this question — the Harvard Health Professionals Follow-up Study, tracking nearly 32,000 men over 18 years — found that men who ejaculated 21 or more times per month were significantly less likely to be diagnosed with prostate cancer than men who ejaculated 4–7 times per month. The study provides the strongest evidence to date of a beneficial role of ejaculation in the prevention of prostate cancer, particularly for low-risk disease.

The proposed mechanisms include suppression of the sympathetic nervous system, reduced tension in prostate tissue, slower division of prostate epithelial cells, and potential effects on gene expression that influence tumour susceptibility. Think of it as flushing the system — regular ejaculation may clear out stagnant secretions, reduce inflammation, and keep the prostate tissue turning over in a healthy way.
The caveat: while some studies show an inverse correlation between ejaculation frequency and prostate cancer risk, others present conflicting findings, and there's no consensus on the underlying biological mechanisms. A 2025 meta-analysis of 29 studies covering over 315,000 men found a positive but non-significant association between sexual intercourse frequency and prostate cancer, suggesting it's specifically ejaculation frequency — not sexual activity more broadly — that matters.
The practical takeaway: regular ejaculation appears to be modestly protective, particularly against low-risk prostate cancer. It's not a substitute for screening, and nobody's prescribing a specific number. But it aligns with the broader sexspan framework — maintaining active sexual function isn't just a quality-of-life issue, it may genuinely be part of keeping the prostate healthy.
Anal Sex, Prostate Stimulation, and Prostate Cancer: What the Evidence Actually Says
Let's address this directly, because it's a question that gets asked quietly and rarely answered properly — by any audience, not just MSM (men who have sex with men).
Does anal sex or prostate massage cause prostate cancer? No. There is no evidence that men who engage in same-sex relationships are at an increased risk of developing prostate cancer. Clinical Oncology A large US cancer registry study found no evidence that sexual orientation, anal sex, or a history of male partners was associated with increased prostate cancer risk. PubMed Central The idea that receptive anal sex or prostate stimulation causes prostate cancer is a myth — and a damaging one, because it discourages blokes from getting screened.
Could prostate stimulation actually be protective? Possibly. If the ejaculation frequency data holds — and the Harvard study didn't distinguish how the ejaculation happened — then any sexual activity that promotes regular ejaculation and prostate drainage may contribute to the protective effect. Prostate massage, whether through anal stimulation or direct external techniques, promotes blood flow and helps clear stagnant prostatic secretions. The mechanism is the same: flushing the system, reducing chronic inflammation, maintaining healthy tissue turnover.
The real risk factor isn't the sex act — it's untreated STIs. A history of gonorrhoea was associated with a modestly elevated prostate cancer risk, but this is driven by chronic prostatic inflammation from infection, not by the sexual activity itself. Safe sex practices — barrier protection, regular STI screening, prompt treatment — eliminate this variable regardless of who you're sleeping with.
A practical note on PSA testing. Vigorous prostate stimulation can significantly affect serum PSA levels. If you engage in receptive anal sex or regular prostate massage, avoid anal stimulation for at least 48 hours before a PSA blood test. Otherwise you risk a falsely elevated result that could send you down an unnecessary investigation pathway.
The Prostate-Friendly Lifestyle
- Regular resistance training and aerobic exercise — reduces inflammation, improves insulin sensitivity, helps BPH symptoms
- Mediterranean dietary pattern — high in vegetables, legumes, fish, tomatoes (lycopene), olive oil; low in processed meat
- Pelvic floor exercises — start now, not after a diagnosis; significantly improves post-treatment continence and sexual recovery
- Avoid prolonged sitting — chronic pelvic congestion drives prostatic inflammation; take regular movement breaks
- Maintain healthy testosterone levels — low T isn't protective and may be associated with more aggressive disease at diagnosis
- Maintain a healthy weight — obesity increases both prostate cancer risk and BPH progression
- Limit alcohol — heavy consumption is associated with increased prostate cancer risk and worsens LUTS
Testosterone and Prostate Cancer: The Myth, Debunked
If you're on or considering testosterone replacement therapy, you've probably heard that testosterone causes prostate cancer. It doesn't. That belief traces back to a 1941 study by Charles Huggins — which Morgentaler later showed was based on a single patient. PubMed Central
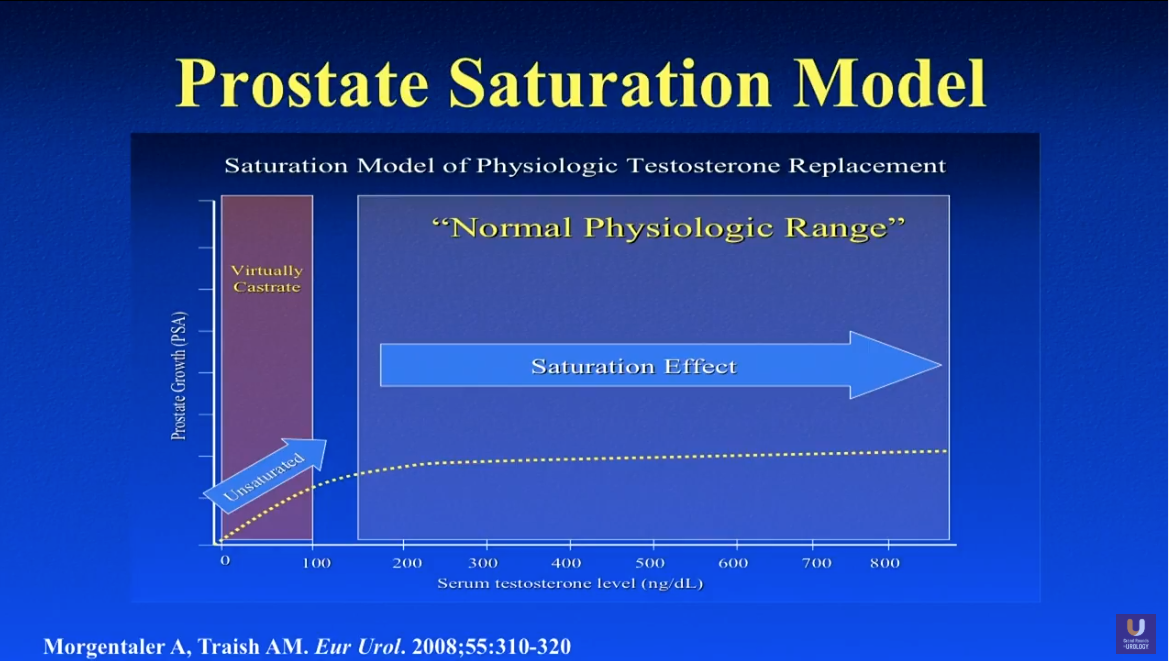
In 2009, Morgentaler formalised the saturation model, proposing that androgen receptors in prostate cells become fully occupied at testosterone levels well below the normal male range (around 200–250 ng/dL), and that raising testosterone above this threshold has no further effect on tumour growth. WJMH Think of watering a garden: bone-dry soil needs water, but once the soil is saturated, more water doesn't make the plants grow taller.
The TRAVERSE study — the largest prospective randomised trial on TRT safety — confirmed that testosterone replacement in carefully screened hypogonadal men does not significantly increase the risk of prostate cancer. WJMH You still need PSA monitoring before and during TRT, but the idea that testosterone causes prostate cancer has been comprehensively debunked.
What You Should Actually Do
Get a baseline PSA. Updated Australian guidelines are recommending a baseline PSA test for men who request it at age 40, with earlier and more frequent testing for those with family history or sub-Saharan ancestry. Usanz If you haven't had one, ask for it.
Don't ignore urinary symptoms. Getting up twice a night to pee isn't a rite of passage. It's a symptom that can be investigated and treated — often with a single daily medication that benefits both your prostate and your sexual function.
If your PSA is elevated, ask about mpMRI before biopsy. The diagnostic pathway has changed. You shouldn't be going straight to a biopsy in 2026 without an MRI first, except in specific clinical circumstances.
If you're on or considering TRT, don't let prostate cancer fear be the reason you avoid it. The evidence doesn't support the old assumption. What the evidence does support is proper screening before and during treatment.
Maintain an active sex life. Regular ejaculation appears to be modestly protective against low-risk prostate cancer. It's not a prescription — but it's one more reason to take your sexual health seriously and address any dysfunction rather than ignoring it.
If you're MSM, screen proactively and advocate for yourself. The functional stakes of late-stage treatment are higher. Close the screening gap. And make sure your treating team knows how you have sex so they can account for it in your care plan.
Know your family history. A family history of prostate cancer doubles your risk. Two or more close male relatives increases it five-fold. Prostate Cancer Foundation Australia If your dad or brother had it, your screening timeline starts earlier and your vigilance needs to be higher.
Prostate cancer is the most commonly diagnosed cancer in Australia. Prostate Cancer Foundation Australia It's hitting younger men at rates we haven't seen before. PCFA But the diagnostic tools are better than ever, the screening guidelines are catching up, and most of what used to terrify men about their prostate — the blind biopsy, the testosterone myth, the idea that sex is somehow part of the problem — has been replaced by smarter, evidence-based approaches.
Your prostate is going to need attention eventually. The question is whether you give it attention on your terms — or on the disease's.
