
The fat you can't pinch is the fat that's quietly wrecking you
Here's a question that should bother you more than your bathroom scales do: where is your fat, actually?
Not how much. Where. Because the bloke with the beer gut and the bloke with the "skinny-fat" dad bod can carry the same number on the scales and have completely different futures. The number doesn't know the difference between fat sitting harmlessly under your skin and fat that's set up camp inside your liver, your pancreas, and the muscles you need to get off the floor when you're eighty. Same weight. Wildly different engine.
This is the part of the GLP-1 conversation nobody's having properly. Everyone's arguing about how much weight Ozempic and Mounjaro strip off, and whether they nuke your muscle along the way. Fair questions. But they're the wrong frame. The interesting story isn't the total weight — it's what these drugs do to where your fat lives, and whether the muscle you keep is better or worse than the muscle you started with.
So let's actually get into it.
Fat is not one thing
Think of body fat like real estate. Subcutaneous fat — the stuff you can pinch on your belly, your love handles, the back of your arms — is the cheap suburban land. It's not pretty, but it's mostly inert. It sits there. It's even a bit protective.
Then there's the fat you can't pinch, and that's where the trouble lives.
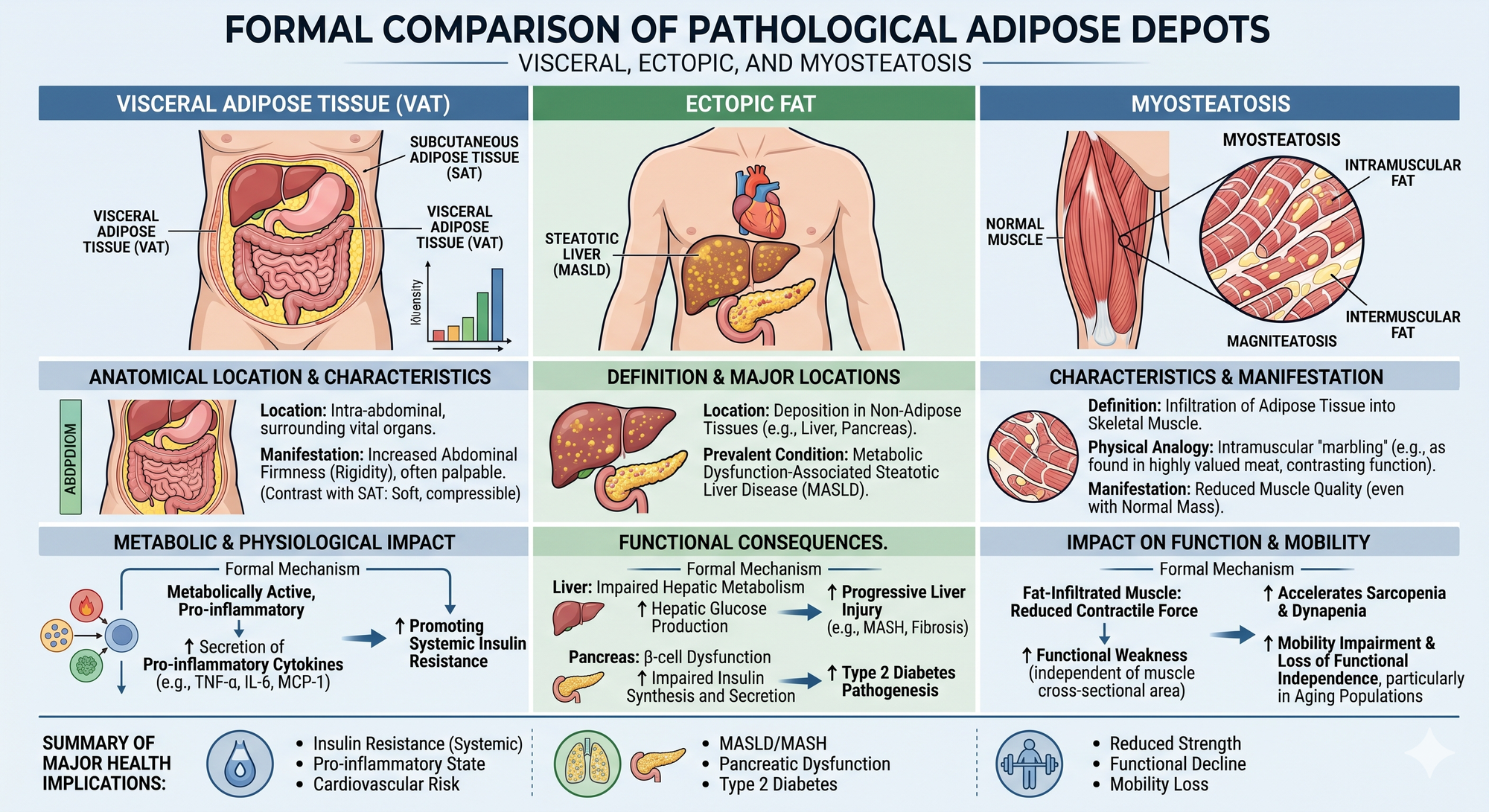
Visceral fat (VAT) is the fat packed in and around your organs, deep in the abdomen. This is the fat that makes a gut feel hard rather than soft. It's metabolically angry — it pumps out inflammatory signals and drives insulin resistance.
Ectopic fat is worse again. "Ectopic" just means "in the wrong place." It's fat that's infiltrated organs that aren't supposed to store it — chiefly your liver and pancreas. Fatty liver (now called MASLD — metabolic dysfunction-associated steatotic liver disease) is the headline act, and it's shockingly common in Australian and New Zealand men carrying extra weight. Fat in the pancreas may quietly sabotage the very cells that produce insulin.
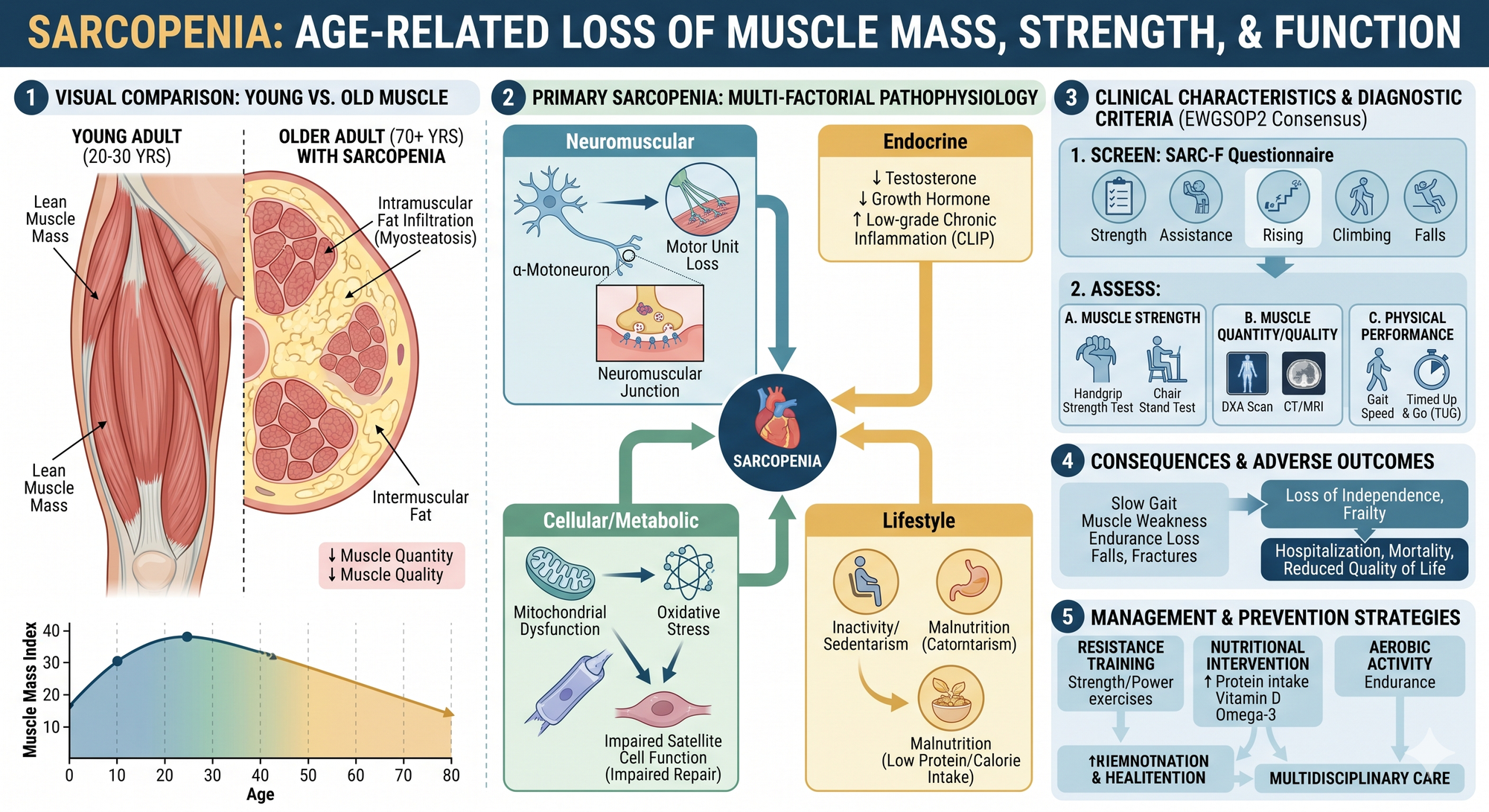
Myosteatosis is the one almost nobody talks about, and it might be the most important for how you actually feel and function. It's fat infiltrating your muscle — marbling, like a wagyu steak. And here's the cruel irony: a well-marbled steak is delicious precisely because it's the opposite of what you want in your own legs. Marbled muscle is weaker muscle. You can have a perfectly normal amount of muscle on a scan and still be weak, because the muscle is shot through with fat that contributes nothing but dead weight.
Myosteatosis directly reduces strength and physical function even when total muscle mass looks fine. It's a major reason people in their sixties and seventies lose the ability to do ordinary things — and it's been hiding in plain sight because the standard tools don't measure it.
Why the scales — and even your DEXA scan — can lie to you

If you've gone down the longevity-clinic path, you've probably had a DEXA scan. It's a good test and I'm glad you did it. But let's be honest about what it can and can't tell you, because the clinics selling them are sometimes less than candid.
DEXA is genuinely excellent at three things: total fat mass, total lean mass, and bone density. If you want to know whether you're losing fat or muscle over time, DEXA tracks it well and the radiation dose is tiny. For most men, it's the right starting tool.
But DEXA has a blind spot, and it's exactly the blind spot that matters for this conversation. It estimates visceral fat rather than measuring it directly, and it essentially cannot see ectopic fat at all. It can't tell you how much fat is in your liver. It can't see the fat in your pancreas. And it's poor at myosteatosis — it lumps the fat marbled inside your muscle into the general "lean mass" pile, so a DEXA can call your muscle healthy when it's quietly turning to wagyu.
For the fat that actually predicts trouble, you need better imaging:
- MRI and MRS (magnetic resonance spectroscopy) are the reference standard. MRI-PDFF — proton density fat fraction — measures liver fat with remarkable accuracy and reproducibility, which is why every serious drug trial uses it. MRI can also map muscle fat infiltration directly. The catch is cost and access: in AU/NZ this is largely research-grade or specialist territory, not something your GP orders for curiosity.
- CT can quantify muscle attenuation (a myosteatosis proxy) and visceral fat, but it carries a real radiation dose, so it's not a casual monitoring tool.
- A tape measure around your waist remains an embarrassingly good proxy for visceral fat, costs nothing, and you already own one.
The honest takeaway: DEXA tells you the quantity story. It doesn't tell you the quality and location story. Don't let a clean DEXA convince you the engine's fine when it's never looked under that particular part of the bonnet.
Where GLP-1s get genuinely interesting
Now the drugs. Semaglutide (Wegovy) and tirzepatide (Mounjaro) are the two that matter here. Both are now Medsafe-approved in New Zealand for weight management — Wegovy from July 2025 — and both are TGA-approved in Australia, with Mounjaro also picking up a sleep-apnoea indication in 2025. Neither is publicly funded for weight loss on either side of the Tasman, which means you're looking at roughly NZD 400–600 a month out of pocket. (In NZ, watch this space: Pharmac's expert advisory group provisionally recommended funding Wegovy with high priority in early 2026, though a recommendation is not a decision.)
The weight-loss numbers are real — around 15% of body weight on semaglutide, north of 20% on tirzepatide at top dose. But forget the total for a second. Here's what these drugs do to the bad fat, and it's where the evidence is strongest.
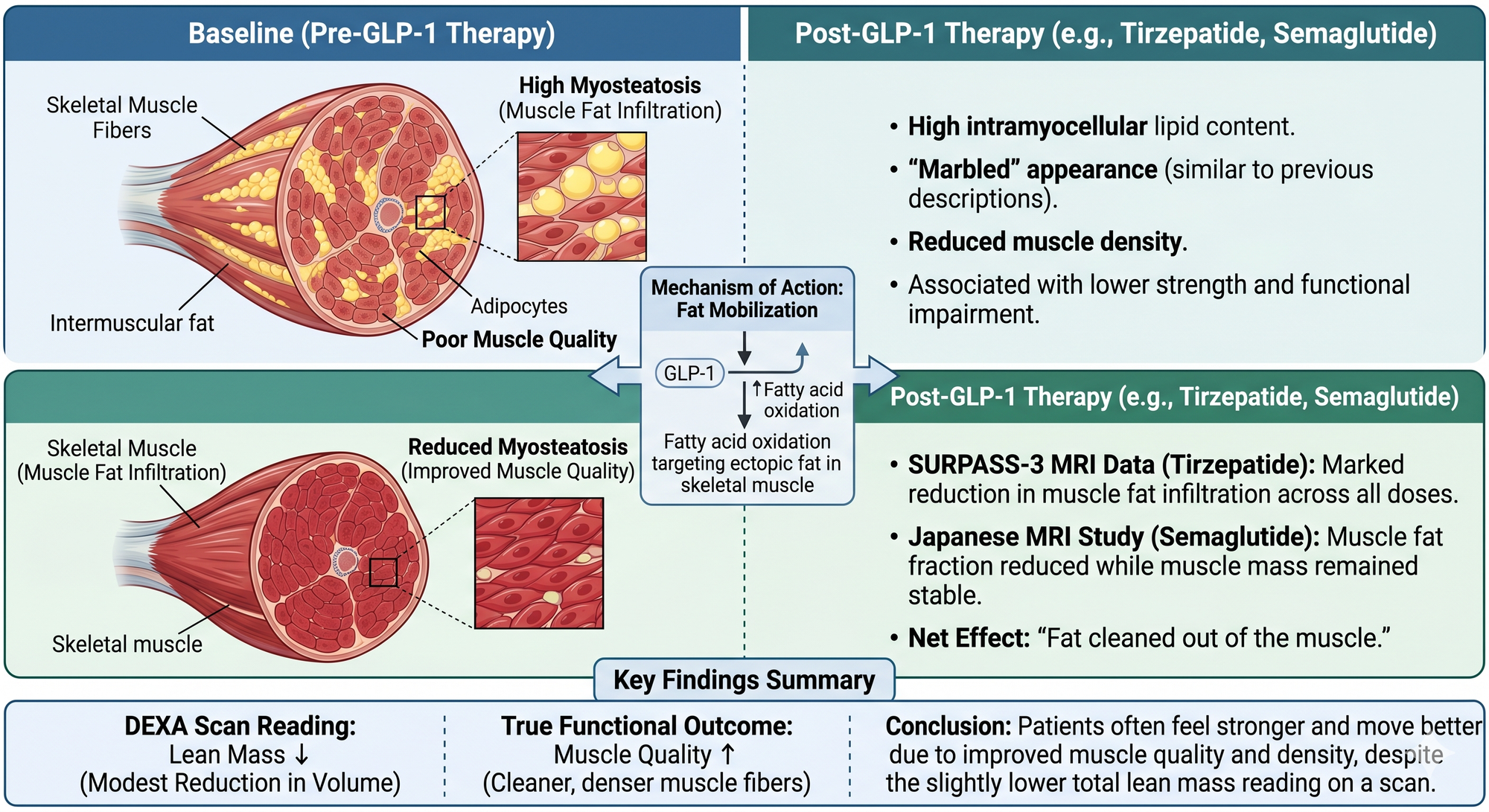
In the SURPASS-3 MRI substudy, tirzepatide cut liver fat content by around 8 percentage points in a year — roughly halving it from a starting point of about 16% — while also significantly shrinking visceral fat. That's not a side effect; that's the engine being cleaned out. Across the MASH trials (SYNERGY-NASH), tirzepatide drove genuine resolution of fatty liver disease confirmed on biopsy. This is some of the most robust evidence in the whole field. If you've got fatty liver — and a lot of you reading this do, whether you know it or not — these drugs reliably reverse it.
The myosteatosis story is newer but pointing the same way. In that same SURPASS-3 imaging work, tirzepatide produced marked reductions in muscle fat infiltration across all doses, while muscle volume only dropped modestly and in proportion to overall weight loss. A separate Japanese study using MRI found semaglutide reduced muscle fat fraction while muscle mass held. Translation: the fat got cleaned out of the muscle, and the muscle that remained was higher quality. That's why a lot of people report feeling stronger and moving better after GLP-1 weight loss, even when a DEXA says their lean mass went down. The number went down; the quality went up.
The catch you have to take seriously
Here's where I stop being a cheerleader, because there's a real cost and the clinics flogging these drugs gloss over it.
GLP-1s strip muscle, not just fat. In the STEP 1 trial, lean mass made up around 40% of the total weight lost on semaglutide. In SURMOUNT-1, tirzepatide's figure was about 25%. That's a wide range, and the honest reading is that somewhere between a quarter and 40% of what you lose on these drugs is not fat.
Now, two things are true at once, and you need to hold both.
The reassuring half: that ratio is roughly what you'd see with any major weight loss, including bariatric surgery and serious dieting. Losing weight always costs some muscle — it always has. And as we've seen, the muscle you keep is often metabolically cleaner. The SURMOUNT-1 investigators argued, fairly, that this isn't disproportionate muscle wasting; it's the normal physiology of getting smaller.
The worrying half: "normal for weight loss" isn't the same as "harmless," especially if you're over fifty, already losing muscle to age, and not doing anything to fight back. Lose 5% of your lean mass on top of the muscle you're already shedding each decade, and you can tip toward genuine weakness. The functional consequences in older adults genuinely aren't fully mapped yet — anyone telling you otherwise is selling something.
So the framing that actually holds up is this: a GLP-1 will clean the fat out of your engine, but it'll also quietly siphon off muscle unless you give your body a reason to keep it. The drug does the fat. You have to do the muscle.
How to not waste the opportunity
If you're on one of these drugs, or thinking about it, the single highest-leverage thing you can do is make the weight you lose the right weight. Two levers, and they're not negotiable:

Lift heavy things, regularly. Resistance training is the signal that tells your body to hang onto muscle while everything else shrinks. This is where "training efficiency" earns its name — you don't need to live in the gym, you need to load your muscles hard enough, two or three times a week, that they have a reason to stay. Bodyweight counts when you're starting; progressing to real load matters as you go. Cardio is great for your heart and does almost nothing to protect muscle. Lifting is the lever.
Eat enough protein. When you're in a deep calorie deficit and barely hungry — which is exactly what these drugs engineer — protein is the first thing to fall off the plate and the last thing you can afford to lose. Make it the thing you eat first at every meal, before the appetite suppression closes the window.
Do those two things and you flip the whole equation. You keep the contractile muscle, you lose the marbling, you reverse the fatty liver, you strip the visceral fat. You come out the other side not just lighter, but with a genuinely better engine — stronger per kilo than when you started.
Skip them, and you'll lose weight and get weaker at the same time. Smaller, softer, and quietly frailer. The scales will be thrilled. Your seventy-year-old self won't be.
The drug is a remarkable tool. But it's a tool for relocating fat out of the places that are killing you — and that only works if you're the one holding onto the muscle while it does. Where your fat lives is the question. These drugs, used properly, are one of the better answers we've ever had. Used lazily, they just make you a smaller version of the same problem.


