
Introduction to ApoB and LDL-C for Dummies
If you've ever had a blood test to check your cholesterol, you've likely heard of "bad cholesterol" (LDL-C). But there's another, arguably more accurate, measure called ApoB. This document will break down what these terms mean, why they matter, and how they relate to your health, in a simple way.
What is Cholesterol and Why Do We Care?
Cholesterol isn't inherently bad—it's a waxy, fat-like substance your body needs to build healthy cells. It travels through your bloodstream inside packages called lipoproteins.
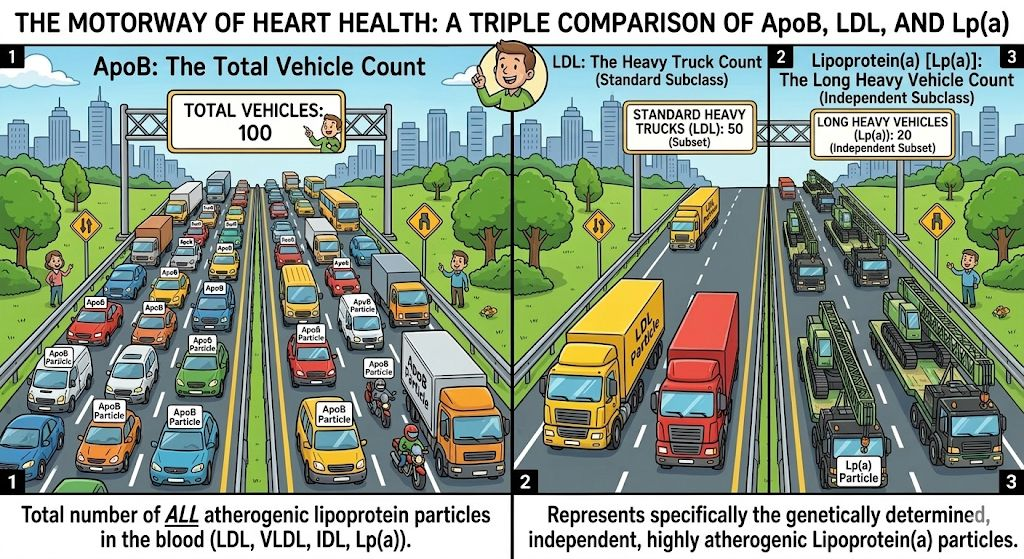
Think of your bloodstream as a highway and cholesterol as building materials. The lipoproteins are the trucks that carry the materials.
There are different types of "trucks," but the most relevant here are:
- Low-Density Lipoprotein (LDL): The "bad" trucks. They deliver cholesterol to your body's tissues. Too many of these can cause traffic jams (plaque) in your arteries.
- High-Density Lipoprotein (HDL): The "good" trucks. They are the cleanup crew, picking up excess cholesterol and taking it back to the liver for disposal.
LDL-C: Measuring Cholesterol in the "Bad Trucks"
LDL-C (Low-Density Lipoprotein Cholesterol) is the measurement of the total amount of cholesterol contained within all the LDL particles ("trucks") circulating in a blood sample.
The Limitation of LDL-C: LDL-C is an estimated value that can sometimes be misleading because LDL particles can vary in size. For instance, a person might have a low total cholesterol weight (low LDL-C) but possess a large number of smaller LDL particles. Since a high count of LDL particles, regardless of size, is a cardiovascular risk, this scenario can be problematic.-----Deeper Dive: Subtypes of LDL Particles
For advanced lipid analysis, LDL is often sub-classified by size and density, which correlates with its atherogenic potential (ability to form plaque). The measurement of ApoB, in contrast to LDL-C, counts all of these LDL particles, regardless of their subtype.Common LDL Particle Subtypes
- Large, Buoyant LDL (Pattern A):
- Characteristics: These particles are larger and less dense.
- Cardiovascular Risk: They are generally considered less harmful because they are less likely to penetrate the arterial wall.
- Small, Dense LDL (sdLDL) (Pattern B):
- Characteristics: These particles are smaller and denser.
- Cardiovascular Risk: Highly atherogenic (more dangerous). Their size allows them to penetrate the artery wall more easily, where they are retained longer and are more susceptible to oxidation—a crucial step in the development of arterial plaque.
ApoB: The Count of the "Bad Trucks"
ApoB stands for Apolipoprotein B.
Each "bad truck" (LDL particle) has a single, unique protein on its surface, like a license plate or a recognizable tag. That tag is the ApoB protein.
Measuring your ApoB level is essentially counting the total number of "bad trucks" in your bloodstream.
Why ApoB is a Better Indicator
ApoB is often considered a better marker for heart disease risk because the true danger comes from the number of harmful particles, not just the amount of cholesterol they carry.
Why? Because for plaque to form, a particle must get into the artery wall. The more particles you have, the higher the chance of one getting stuck and starting the plaque buildup process.
Summary Comparison
This table summarizes the two key measurements:
Next Steps
If you want to discuss your ApoB and LDL-C levels, schedule a consultation with your healthcare provider. You can use this link to book an appointment: Calendar event.
You can review a copy of your recent blood work results here: File.
Remember, a healthy lifestyle—diet and exercise—is the foundation for keeping both your ApoB and LDL-C levels in a healthy range. Consult a dietitian at Place for personalized advice.
Note on Other Lipoproteins: HDL and Triglycerides
While LDL and ApoB are the primary focus for cardiovascular risk assessment, two other components of the standard lipid panel provide additional critical information:
- High-Density Lipoprotein (HDL): As the "cleanup crew" (discussed earlier), HDL particles remove cholesterol from the arteries and transport it back to the liver. High levels of HDL-C are generally protective, leading to its nickname, "good cholesterol." However, the function of the HDL particles (their ability to effectively clean up) may be more important than just the total cholesterol mass they carry.
- Triglycerides (TGs): These are the most common type of fat in your body. They are transported in particles like Very-Low-Density Lipoprotein (VLDL) and Intermediate-Density Lipoprotein (IDL). ApoB measures both VLDL and IDL particles. High triglyceride levels are often associated with metabolic syndrome, insulin resistance, and an increased presence of the highly atherogenic small, dense LDL (sdLDL) particles. A high ApoB, especially when accompanied by high triglycerides, suggests a high number of these dangerous particle types.
Algorithmic Patterns for Cardiovascular Risk Assessment
The fundamental principle is that ApoB (particle count) is the primary driver of risk, and the other lipid components modify that risk.
1. Very Low Risk (Optimal)
- Conditions: Low ApoB + Low LDL-C + Low Triglycerides (TG) + High HDL-C
- Implication: Minimal atherogenic particles, strong protective factors.
2. Classic High Risk (Atherogenic)
- Conditions: High ApoB + High LDL-C
- Implication: A large number of harmful particles carrying a high cholesterol load. Risk is even higher if HDL-C is low and/or TG are high.
- An LDL-C >4.9 mmol/L strongly suggests Familial Hypercholesterolemia (FH), requiring immediate, aggressive therapy due to very high lifetime risk.
3. Discordant High Risk (ApoB Dominant)
- Conditions: High ApoB BUT Low/Normal LDL-C + High TG
- Implication: This is a crucial pattern. The low LDL-C is misleading. High ApoB and high TG indicate a proliferation of small, dense, highly atherogenic particles (sdLDL and VLDL remnants). This is often associated with metabolic syndrome/insulin resistance. Particle count (ApoB) overrules mass (LDL-C).
4. High LDL-C, Lower Risk
- Conditions: Low ApoB BUT High LDL-C
- Implication: The high mass (LDL-C) is due to a small number of large, buoyant, less harmful LDL particles (Pattern A). Since the particle count (ApoB) is low, the overall risk is lower than expected for the LDL-C level.
- Treatment threshold - Treatment for high LDL-C is primarily driven by a patient's overall cardiovascular risk profile, not a single absolute threshold.
- An LDL-C >4.9 mmol/L strongly suggests Familial Hypercholesterolemia (FH), requiring immediate, aggressive therapy due to very high lifetime risk.
5. Residual Risk
- Conditions: High ApoB + LDL-C On Target (e.g., post-statin treatment)
- Implication: Even with effective lowering of cholesterol mass (LDL-C), if the particle count (ApoB) remains high, there is a persistent, significant risk. This is common if underlying metabolic issues (high TG, low HDL-C) are not resolved.
6. Extreme Hypertriglyceridemia Risk
- Conditions: Very High TG + High ApoB + Very Low HDL-C
- Implication: Massive burden of VLDL and remnant particles, which are highly atherogenic. This pattern carries a very high cardiovascular risk.
- The treatment threshold for hypertriglyceridemia is largely defined by the risk of acute pancreatitis, not cardiovascular disease with 5.6mmol/L is required to reduce pancreatitis


