
Your VO2 Max Isn't an Athlete's Number. It's Your "How Long Can I Keep Doing This" Number.
Here's the conversation I have at least once a week.
A bloke in his 50s — let's say he runs a successful business, hasn't been short of breath a day in his life gets a VO2 max reading off his watch or a longevity clinic. The number comes back, say, 34. He shrugs. "I'm not running marathons, mate. Why do I care about some athlete stat?"
Fair question. And the honest answer is that VO2 max has a branding problem. It got famous through endurance sport — cyclists comparing numbers, runners chasing a 60 — so most men file it next to lactate thresholds and carbon-fibre shoes. Stuff for people who race. Not for them.
That's the wrong frame, and it's costing people. Because VO2 max isn't really a performance number. It's a reserve number. It's the size of the gap between what your day demands of you and what your body can actually deliver. And that gap is the quiet thing that decides — decades from now — whether you're the 75-year-old still digging the garden and chasing grandkids, or the one who needs a rest halfway up the driveway.
Let me reframe it properly, then give you three honest ways to use the number depending on who you are.
What the number actually is
VO2 max (say it "vee-oh-two max") is the maximum amount of oxygen your body can take in and actually use during all-out effort, measured in millilitres per kilo of bodyweight per minute. Think of it like the engine in a ute. A bigger engine doesn't mean you're always flooring it — most of the time you're cruising. But it means that when the road tilts uphill, you've got something in reserve. You can tow the load. You don't redline just getting up the hill.
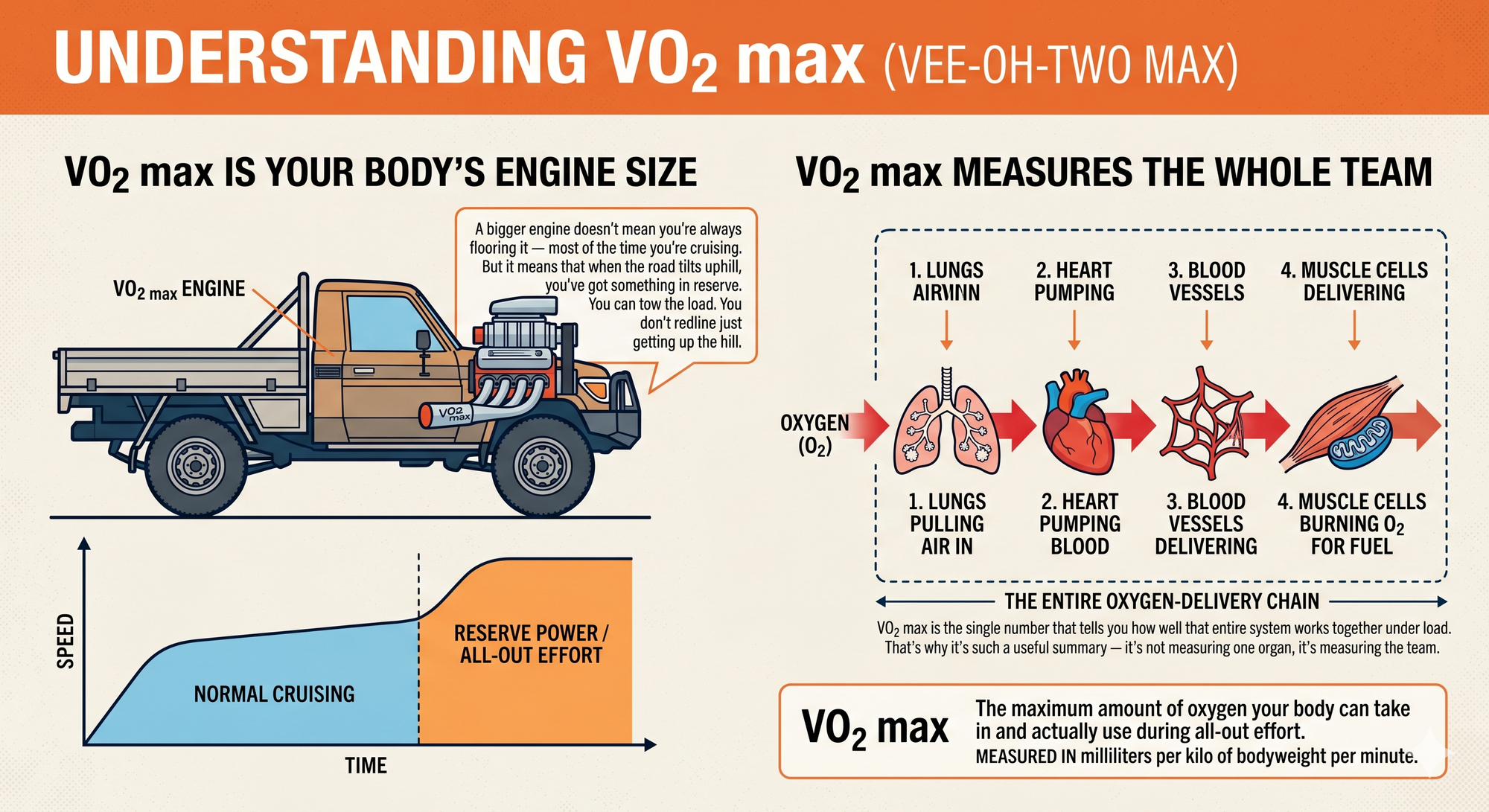
Your "engine" here is the whole oxygen-delivery chain: lungs pulling air in, heart pumping blood, blood vessels delivering it, and muscle cells burning the oxygen for fuel. VO2 max is the single number that tells you how well that entire system works together under load. That's why it's such a useful summary — it's not measuring one organ, it's measuring the team.
And here's the part that surprises people. In a study of 122,007 patients at the Cleveland Clinic, cardiorespiratory fitness was inversely linked to dying from any cause — and there was no upper limit to the benefit. The fitter you were, the longer you lived, with no point where it stopped paying off. A separate analysis of more than 750,000 US veterans found that each one-MET improvement in fitness — roughly 3.5 ml/kg/min of VO2 max — was associated with a 13 to 15% drop in mortality risk, regardless of age, weight or existing illness.
To put that in perspective: being in the lowest-fitness group carried a bigger mortality risk than being a smoker, a diabetic, or having established coronary disease. Low fitness isn't a soft "should probably exercise more" risk factor sitting below the real ones. On this data, it's near the top of the list. It just doesn't get a scary letter from your insurer.
The reframe: VO2 max as your activity floor
Forget elite athletes for a second. Here's the idea that makes this number matter to everyone.
Every physical thing you do has an oxygen cost. Not just running — everything. Walking the dog, carrying shopping up a flight of stairs, mowing the lawn on a warm day, dancing at a wedding, sex, getting off the floor after playing with the grandkids. Each of those has a rough VO2 cost, and if your VO2 max sits comfortably above it, the activity feels easy. When your max drops close to the cost of the task, that task starts to feel like hard work. When your max falls below it, you simply can't do it anymore — or you can't do it without stopping to recover.
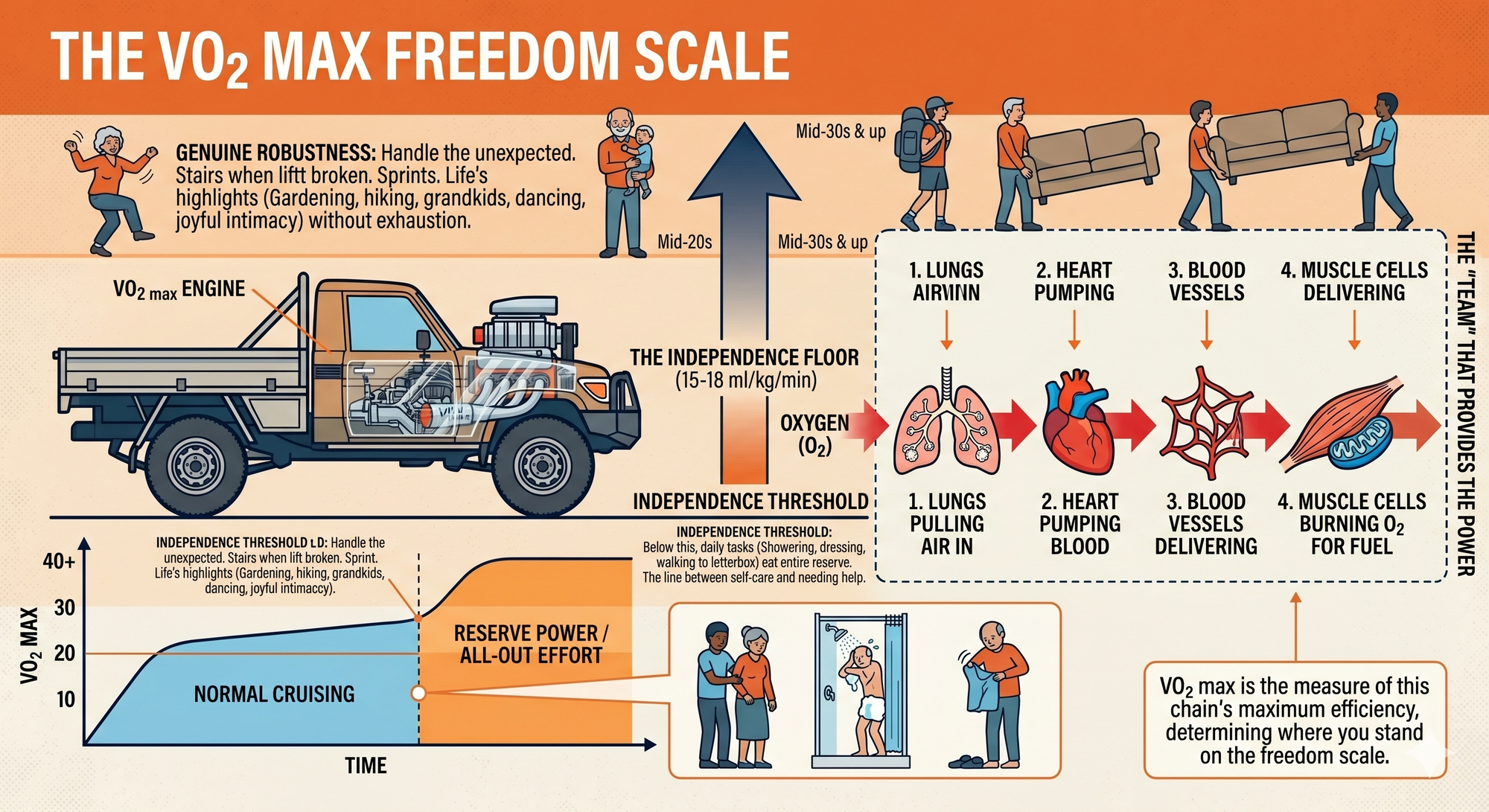
So your VO2 max sets a floor under your independence. Roughly:
- Around 15–18 ml/kg/min is the threshold for living independently. Below that, daily tasks — showering, dressing, walking to the letterbox — start eating your entire reserve. This is the line between managing your own life and needing help with it.
- Mid-20s to low-30s covers most of what makes life worth living for an older adult: gardening without wrecking yourself, having enjoyable sex, a hike on rolling hills, energetic dancing, keeping up with active kids.
- Mid-30s and up is genuine robustness — the capacity to handle the unexpected. A flight of stairs when the lift's broken. Carrying a mate's couch up to a third-floor flat. A sudden sprint for the bus.
Now layer on the uncomfortable bit: VO2 max declines by roughly 1% per year from around your thirties onward, and the decline accelerates after 60. That's not a reason to despair — it's a reason to do the maths. If you're 50 with a VO2 max of 35, and you do nothing, you're looking at the high-20s by 70 and the low-20s by 80. That's not abstract. That's the difference between hiking the Tongariro Crossing at 70 and getting winded on a flat coastal walk.

This is where the "you are here" picture earns its place. The activities you take for granted today each have a future expiry date baked into your current trajectory — unless you change the slope. Moderate hiking might "expire" in your late fifties. Energetic dancing not long after. Slow dancing at a wedding might hold out into your nineties, because it costs almost nothing. The whole point of training your VO2 max isn't to win anything. It's to push every one of those expiry dates further out — ideally past the point where anything else gets you first.
That's the number's real job. Not a podium. A floor that stays high enough, for long enough, that you get to keep your life.
Where do you actually sit? (And a word on the watch)
Knowing your number matters, because the reframe only works if you can see your trajectory. Three ways to get it, in descending order of accuracy:
The lab test (the gold standard). You run or cycle to exhaustion wearing a mask that measures every breath. Ten to twenty minutes, genuinely unpleasant for the last two, and the most accurate reading you'll get. In Australia, exercise physiology labs and sports clinics charge roughly $185 to $360. In New Zealand, private labs like AUT Human Potential Clinic in Auckland offer gas-analysis testing. Worth doing once if you want a true baseline, or if you've got cardiac risk factors and want it done with supervision.
Your smartwatch (good enough for tracking). Apple Watch, Garmin and the like estimate VO2 max from your heart rate and pace. They're not lab-accurate in absolute terms — one fellow compared his Apple Watch (38.6–39.6) against a lab result (39.4) and they nearly matched, but exercise physiologists will tell you they've also seen watches off by a country mile. The trick: don't obsess over the exact figure, watch the trend. If your watch says 38 and three months of training nudges it to 41, that direction is real and useful, even if the true number is a point or two off. The watch is a bathroom scale, not a blood test — useful for tracking, not for diagnosis.
The submaximal estimate. Your GP or exercise physiologist can estimate it from a graded test without pushing you to absolute exhaustion. Less precise, but safer for someone deconditioned or with heart concerns, and a sensible starting point if you've been off the tools for years.
Match your reading against age and sex norms (the classification tables from the Cleveland Clinic data are the standard reference). But don't get lost in the percentile. The more useful question isn't "what's my rank?" — it's "where's my floor, and which way is it heading?"
Three ways to use the number
If you're an athlete or weekend warrior: optimise it
You already care about the number, so I'll be brief. VO2 max responds best to time spent near your ceiling. The most-studied tool is the Norwegian 4x4: four minutes hard (around 85–95% of max heart rate — hard enough that you can't hold a conversation), then three minutes easy, repeated four times, after a warm-up. In Helgerud's foundational study, three sessions a week for eight weeks lifted VO2 max by 7–9% in already-trained subjects, clearly beating moderate steady-state work.
But intervals sit on top of a base, not instead of one. The endurance world's open secret is that most of the volume should be easy — Zone 2, conversational pace, the stuff that builds the mitochondrial and vascular machinery the hard sessions then sharpen. Hard days hard, easy days genuinely easy. The grey middle — moderately uncomfortable all the time — is where a lot of keen amateurs plateau.
If you're the average bloke who isn't training: protect the floor
This is most men, and the message is the one with the biggest payoff. You don't need to chase elite numbers. You need to not be in the bottom group — because that's where the risk is concentrated.
Here's the most encouraging finding in this entire field: simply moving from the lowest fitness category to the next one up — "below average" — was associated with roughly a halving of ten-year mortality in the Cleveland data. The biggest single gain in the whole dataset is the first step off the floor. You do not have to become an athlete. You have to stop being unfit.
Practically: build a base of easy aerobic work you'll actually sustain — brisk walking, cycling, swimming — most days. Then, once that's a habit and your GP's given you the nod, add one harder session a week. It doesn't have to be a formal 4x4. Walking hills hard. A few uphill efforts on the bike. Stairs instead of the lift, done with intent. The first bit of intensity in a previously sedentary life is where the VO2 max needle moves fastest. This is also exactly the cohort our [cardiovascular health articles] are written for — the same training that lifts your VO2 max is the training that keeps your arteries honest.
If you're older (or training a parent): it's the most modifiable thing you've got
This is where I get genuinely evangelical, because the assumption that high-intensity exercise is "for the young" is wrong, and it's costing older people their independence.
The Generation 100 study put this to the test properly: more than 1,500 Norwegians aged 70 to 77, randomised, training for five years. The high-intensity interval group — yes, 4x4 intervals, in seventy-somethings — got greater VO2 max improvements than the moderate group, with high quality of life and a strong safety record. People in their seventies improved a number most assume only falls.
The caveats are real and I won't gloss them: the intervals were adapted, progressed slowly, and done by people cleared to exercise hard. If you or your parent has heart disease, uncontrolled blood pressure, or has been sedentary for years, this starts with a GP visit and ideally an exercise physiologist, not a YouTube video. But — and this is the part that matters — the ceiling for improvement is far higher than almost anyone believes. A deconditioned 70-year-old who builds an aerobic base and then adds carefully progressed intensity can claw back years of decline. Every point of VO2 max regained is an activity rescued from that expiry list.
There's one more piece the cardio-only crowd misses. VO2 max is oxygen used per kilo of bodyweight. Two things move that ratio: the oxygen on top, and the body on the bottom. Losing muscle as you age — sarcopenia — quietly shrinks the engine and weakens the pump that gets you off the floor and up the stairs in the first place. Which is why strength training isn't a separate project from your VO2 max; it protects the denominator and the machinery both. The older you are, the more the two have to be done together. Cardio buys you the reserve; strength buys you the ability to use it.
The bottom line
Stop thinking of VO2 max as a score and start thinking of it as a slope. Today's number matters far less than where the line is heading and how high the floor stays under it.
You don't need to race anyone. You need enough reserve that the things you love — the garden, the hill, the dance floor, the grandkids — stay inside your capacity for as long as you're around to enjoy them. That's not vanity and it's not athletics. It's the most concrete longevity decision you can actually act on, and unlike your genes or your postcode, it's one you get to change.
Find your number. Watch the trend. Then bend the slope.
This article is general information, not personal medical advice. If you've got cardiac risk factors, existing heart disease, or you've been inactive for a long stretch, talk to your GP before starting high-intensity exercise — and consider getting that baseline test done under supervision.


