
Your Testosterone Blood Test, Decoded. Here's what all these numbers mean, and how they talk to one another.
Your GP ordered a "hormone panel" and you've got a printout full of abbreviations and reference ranges. Most blokes look at the testosterone number, decide whether it's "good" or "bad," and ignore the rest. That's like checking the oil in your car and ignoring the coolant, brake fluid, and fuel gauge.
Testosterone doesn't operate in isolation. It's part of an interconnected system where your brain, liver, thyroid, adrenal glands, and fat tissue all influence each other. Understanding the full panel — even at a basic level — helps you have a much more useful conversation with your doctor.
Here's the map of how these biomarkers connect, followed by a plain-English explanation of each one.
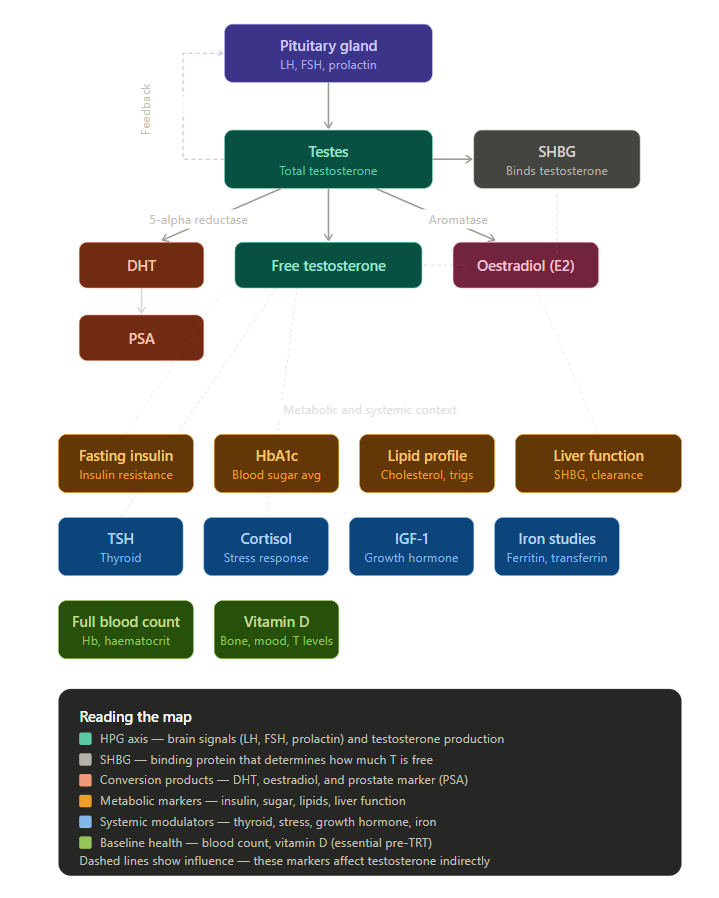
The HPG Axis: Your Hormonal Command Chain
LH and FSH are hormones released by your pituitary gland (a pea-sized structure at the base of your brain). LH (luteinising hormone) tells your testes to produce testosterone. FSH (follicle-stimulating hormone) drives sperm production. If your testosterone is low, the first question is why — and LH/FSH tell you where the problem sits. High LH with low testosterone means the testes aren't responding to the signal. Low LH with low testosterone means the brain isn't sending the signal in the first place. Completely different problems, completely different approaches.
Prolactin is also released by the pituitary and is worth checking on a male hormone panel. Elevated prolactin directly suppresses LH, which in turn suppresses testosterone production. Causes range from stress and certain medications (particularly antipsychotics and some antidepressants) to, rarely, a pituitary adenoma (a small benign tumour). If your testosterone is low and your LH is also low, prolactin helps determine whether the pituitary itself is the problem.
Total testosterone is the headline number — everything your testes produce. But most of it (roughly 98%) is bound to proteins in your blood and isn't biologically active.
Free testosterone is the 2% that's unbound and actually available for your body to use. You can have a "normal" total testosterone but low free testosterone if your binding proteins (especially SHBG) are elevated — which is why testing both matters.
The Gatekeeper
SHBG (sex hormone-binding globulin) is the protein that binds to testosterone in your bloodstream, making it unavailable for your body to use. Think of SHBG as the bouncer at the door — the more bouncers, the less testosterone gets through to do its job. SHBG is produced by the liver and is influenced by almost everything in the metabolic panel: insulin resistance drives it down (paradoxically increasing free T but in a metabolically unhealthy context), while thyroid hormone, ageing, and liver disease drive it up. It's the single most important bridge between the hormonal and metabolic sides of your blood test.
The Conversion Products
Testosterone doesn't just sit there. Your body converts it into two other hormones that matter:
DHT (dihydrotestosterone) is produced via an enzyme called 5-alpha reductase. It's the more potent androgen — responsible for male-pattern hair distribution, prostate growth, and (less helpfully) hair loss. If you're on finasteride for hair loss, it works by blocking this conversion.
Oestradiol (E2) is produced via an enzyme called aromatase, which converts testosterone into oestrogen. Yes, men need oestrogen — it's essential for bone density, brain function, and joint health. But too much (often driven by excess body fat, since fat tissue is rich in aromatase) can suppress testosterone production, cause breast tissue development, and affect mood. The balance between testosterone and E2 is as important as the absolute numbers.
PSA (prostate-specific antigen) isn't a hormone, but it's essential baseline data — particularly if testosterone replacement therapy (TRT) is being considered. PSA is a marker of prostate activity, and while an elevated PSA doesn't necessarily mean cancer, it needs to be assessed before any testosterone treatment begins, since TRT can stimulate prostate tissue. Think of it as a pre-flight check: you want to know the baseline before anything changes.
The Metabolic Context
This is where most "hormone clinics" stop reading and where a proper assessment starts.
Fasting insulin measures how hard your pancreas is working to manage blood sugar. Elevated fasting insulin — even with normal blood glucose — is an early sign of insulin resistance, which directly suppresses testosterone production and increases aromatase activity (more T converted to E2). It's one of the most underappreciated drivers of low testosterone in overweight men.
HbA1c gives you a three-month average of blood sugar control. It's the metabolic trend line. Elevated HbA1c alongside high fasting insulin tells you insulin resistance is already established.
Lipid profile (total cholesterol, LDL, HDL, triglycerides) matters because cholesterol is literally the raw material your body uses to make testosterone. But the lipid panel's main role here is cardiovascular risk assessment — because the same vascular health that drives heart disease also drives erectile dysfunction.
Liver function tests (LFTs) are relevant because the liver produces SHBG (the protein that binds testosterone and reduces your free T). Liver disease, fatty liver, and alcohol use all affect SHBG levels — and therefore how much of your testosterone is actually available. The liver also metabolises and clears hormones, so impaired liver function can skew the entire panel.
The Systemic Modulators
TSH (thyroid-stimulating hormone) is your thyroid screening marker. Both hypothyroidism (underactive) and hyperthyroidism (overactive) directly affect testosterone, SHBG, and energy metabolism. An undiagnosed thyroid problem can mimic low testosterone symptoms almost perfectly — fatigue, weight gain, low mood, poor libido. Checking TSH rules this out.
Cortisol is your primary stress hormone. Chronically elevated cortisol (from sustained psychological stress, poor sleep, overtraining, or illness) directly suppresses the HPG axis — your brain literally deprioritises reproduction when it thinks you're under threat. If your testosterone is low and your cortisol is high, the hormonal problem may actually be a stress problem.
IGF-1 (insulin-like growth factor 1) is a proxy marker for growth hormone activity. It's relevant to body composition, muscle recovery, and tissue repair. Low IGF-1 alongside low testosterone can point toward pituitary dysfunction. In the longevity space, the relationship between IGF-1 and ageing is complex — but for a baseline male health panel, it rounds out the anabolic picture.
Iron studies (ferritin, transferrin saturation, serum iron) matter more than most blokes realise. Iron overload (haemochromatosis — common in men of Northern European descent, and very common in Australia/NZ) can damage the pituitary gland and suppress testosterone production. It's one of the most treatable causes of secondary hypogonadism and one of the most frequently missed. Conversely, iron deficiency causes fatigue that overlaps with low-T symptoms.
Baseline Health Markers
Full blood count (FBC) — specifically haemoglobin and haematocrit — is non-negotiable if TRT is anywhere on the horizon. Testosterone stimulates red blood cell production, and one of the most common side effects of TRT is polycythaemia (too many red blood cells), which thickens the blood and increases the risk of clots. Your pre-treatment haemoglobin and haematocrit establish the baseline that your doctor will monitor against. Even without TRT, FBC can reveal anaemia (which mimics low-T fatigue) or elevated red cells from other causes.
Vitamin D has been increasingly linked to testosterone levels, mood, bone density, and immune function. Deficiency is remarkably common in Australia and New Zealand despite the sunshine — particularly in blokes who work indoors, have darker skin, or live in the southern states during winter. Low vitamin D doesn't directly cause low testosterone, but correcting a deficiency has been associated with modest improvements in T levels, and it overlaps heavily with the fatigue-low mood-poor recovery symptom cluster that brings most men to get tested in the first place.
Why the Full Panel Matters
A testosterone number without context is like a blood pressure reading without knowing someone's age, weight, or medication history. The point of testing all of these together is to understand the system, not just the headline.
A bloke with low testosterone, high fasting insulin, elevated liver enzymes, and a BMI of 34 doesn't need testosterone replacement — he needs metabolic intervention. A bloke with low testosterone, high LH, and normal everything else might have primary testicular failure. A bloke with low testosterone, low LH, high cortisol, and poor sleep has a hypothalamic-pituitary suppression problem that no amount of testosterone gel will fix until the underlying cause is addressed.
The blood test gives you the map. Your GP or specialist reads it as a system. That's the conversation worth having.
Piecing the Patterns Together
Once you understand the system, common conditions jump off the page:
Primary testicular failure — low total T, low free T, high LH/FSH (brain screaming at testes that aren't responding), normal prolactin.
Hypothalamic hypogonadism — low total T, low free T, low LH/FSH (brain isn't sending the signal), elevated cortisol or low energy intake often the culprit.
Pituitary adenoma — low total T, low LH/FSH, high prolactin (tumour producing excess prolactin which suppresses everything downstream).
Metabolic suppression — low-normal total T, low free T, low SHBG, high fasting insulin, elevated HbA1c, poor lipid profile (insulin resistance dragging the whole system down — the most common pattern in overweight men over 40).
Your GP reads these like a mechanic reads fault codes — the combination tells the story, not any single number.

