
10 health issues to consider before considering further treatment

Testosterone replacement therapy (TRT) has become one of the most talked-about treatments in men’s health. And for good reason — when used appropriately, it can be transformative. But here’s what often gets lost in the conversation: many of the symptoms that lead men to consider TRT are driven by fixable, upstream health issues that have nothing to do with testosterone itself.
Fatigue, low libido, brain fog, irritability, poor recovery from exercise, weight gain around the middle — these are real symptoms, and they deserve proper attention. But jumping straight to TRT without addressing the foundations is a bit like putting premium fuel in a car with flat tyres. You might get a small boost, but you’re not going to fix the ride.
Before reaching for the prescription pad, here are ten health issues worth optimising first. Addressing these may resolve your symptoms entirely — or, if TRT is ultimately warranted, ensure you get the best possible response from treatment.
TRT is a lifetime commitment and may not suit everyone. Where less invasive and more affordable sustainable strategies may be equally effective.
Table of Contents
- Sleep Quality, Duration, and Obstructive Sleep Apnoea
- Body Composition: Visceral Fat and Muscle Mass
- Insulin Resistance and Metabolic Health
- Exercise and Physical Activity
- Alcohol and Substance Use
- Mental Health: Depression, Stress, and Anxiety
- Iron Studies and Haematology
- Key Micronutrients: Vitamin D, Magnesium, and Zinc
- Prioritise Sexual Health and Your Relationship
- Environmental Endocrine Disruptors
1. Sleep Quality, Duration, and Obstructive Sleep Apnoea
If there’s one thing that deserves top billing, it’s sleep. Testosterone is produced in a pulsatile fashion, with the majority of daily secretion happening during deep sleep. Chronic sleep deprivation — even modest reductions to five or six hours a night — can suppress testosterone levels by 10–15%, which is roughly equivalent to ageing 10 to 15 years hormonally.
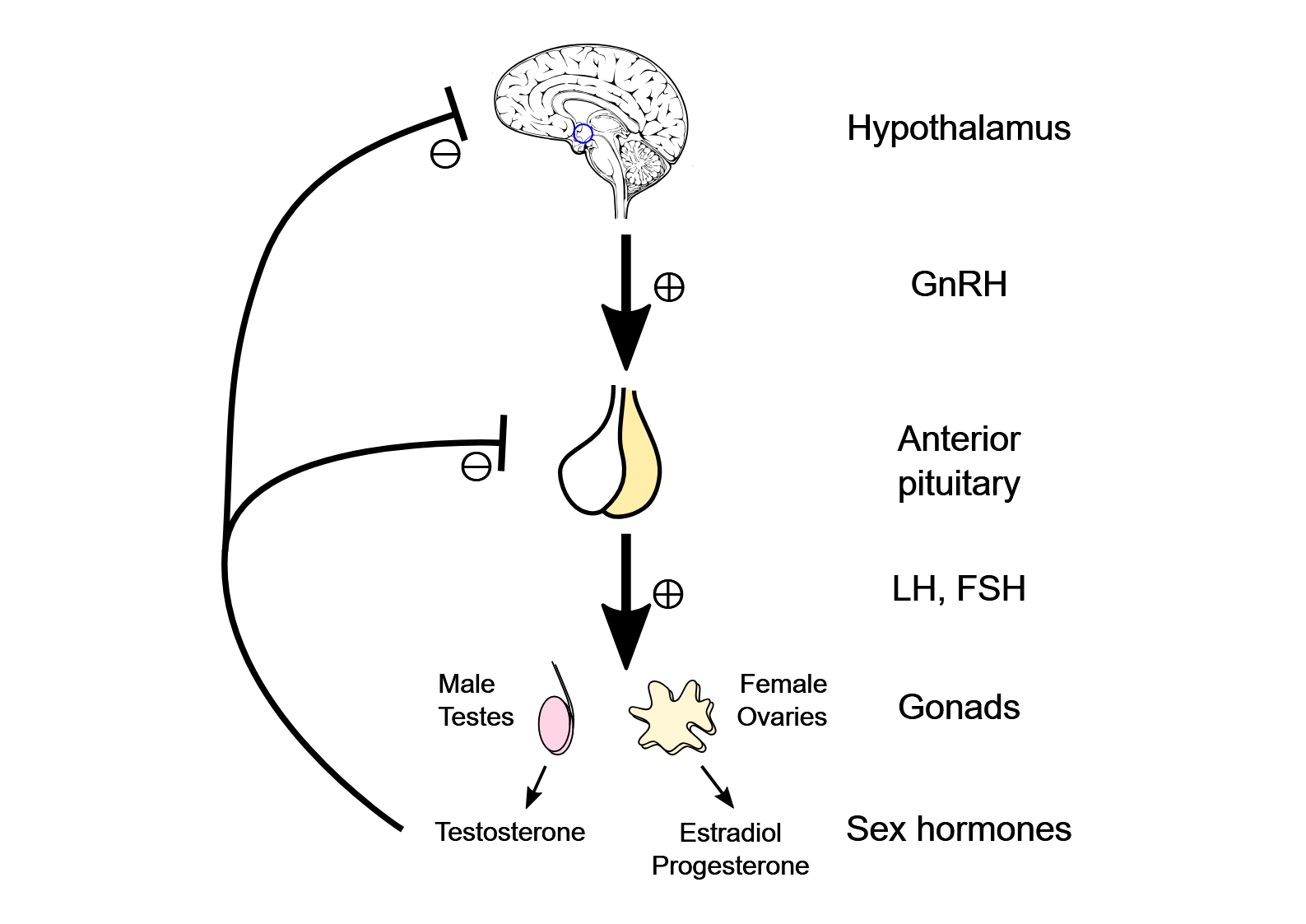
And it’s not just about hours. Poor sleep architecture (fragmented sleep, reduced slow-wave sleep, excessive light exposure before bed) can impair the hypothalamic-pituitary-gonadal axis even when total sleep time looks adequate on paper.
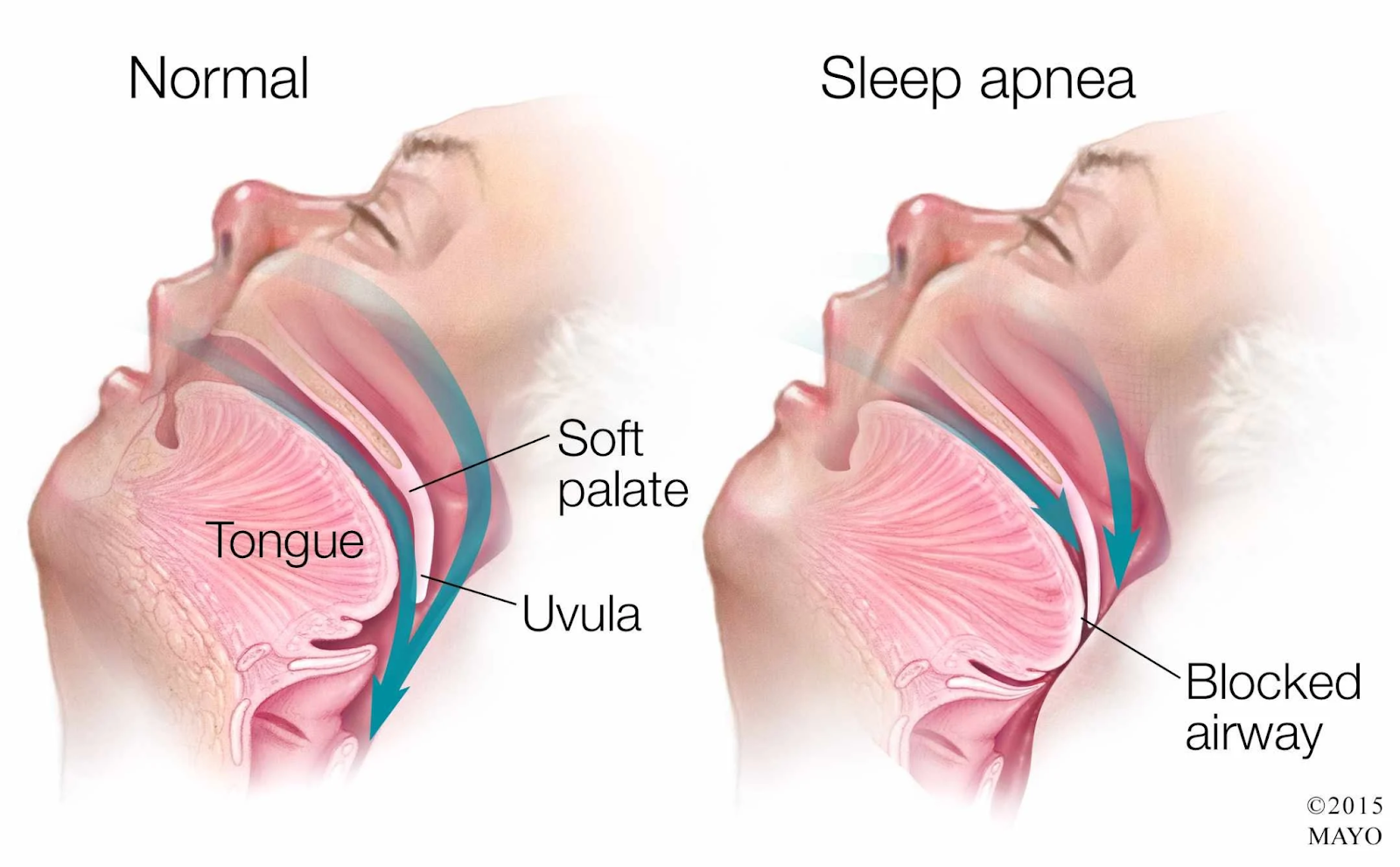
One of the most important — and most underdiagnosed — disruptors of sleep quality is obstructive sleep apnoea (OSA). OSA causes repeated drops in oxygen during sleep, fragmenting sleep architecture and suppressing the nocturnal testosterone surge. It also promotes insulin resistance, weight gain, and cardiovascular risk, compounding the hormonal damage. OSA is both a cause and a consequence of low testosterone, creating a vicious cycle that won’t break without targeted treatment.
Importantly, starting TRT in a man with undiagnosed OSA can actually worsen the condition. Testosterone can increase upper airway collapsibility and raise haematocrit (red blood cell concentration), both of which exacerbate apnoea. This is why screening for OSA before initiating TRT is not optional — it’s essential.
What to do:
• Aim for 7–9 hours of quality sleep per night, consistently.
• Prioritise sleep hygiene: dark room, cool temperature, consistent wake time.
• Limit screens and blue light in the hour before bed.
• If you snore, wake with headaches, feel unrefreshed despite adequate sleep, or your partner has witnessed you stopping breathing at night — get a sleep study. Home-based sleep studies are now widely available and Medicare-rebatable in Australia.
• If OSA is confirmed, treatment with CPAP or a mandibular advancement device often improves testosterone, energy, mood, and metabolic markers significantly.
Think of sleep as the tide that lifts all hormonal boats. And if that tide keeps going out despite your best efforts, check for OSA — it’s like trying to fill a bath with the plug out.
2. Body Composition: Visceral Fat and Muscle Mass
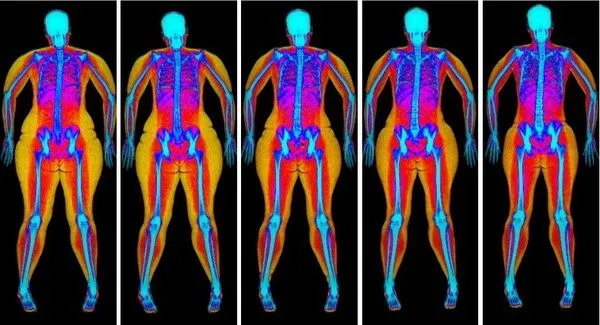
Excess body fat — particularly visceral fat stored around the organs — is one of the most potent suppressors of testosterone. Fat tissue contains the enzyme aromatase, which converts testosterone to oestradiol (oestrogen). The more visceral fat you carry, the more testosterone you lose to this conversion, creating a vicious cycle: low testosterone promotes fat gain, and fat gain further lowers testosterone.
At the same time, low muscle mass (sarcopenia) reduces your metabolic rate and your body’s sensitivity to anabolic signals. It’s not just about the number on the scale — it’s about the ratio of lean mass to fat mass.
What to do:
• Get a body composition assessment — a DEXA scan is the gold standard and gives you visceral fat area, lean mass by region, and bone density in one hit.
• Even a 5–10% reduction in body fat can meaningfully improve testosterone levels.
• Prioritise resistance training to build and preserve lean mass (see Section 4).
Many men who present with ‘low testosterone’ actually have normal production that’s being hijacked by excess aromatase activity in visceral fat. Lose the fat, and the testosterone often comes back on its own.
3. Insulin Resistance and Metabolic Health
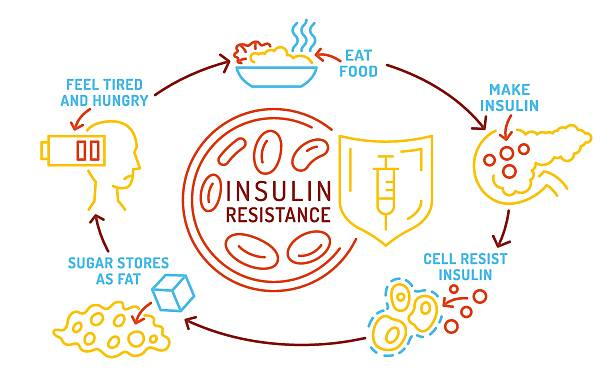
Insulin resistance is the metabolic elephant in the room. When your cells stop responding efficiently to insulin, your body compensates by producing more of it. Chronically elevated insulin (hyperinsulinaemia) suppresses sex hormone-binding globulin (SHBG), disrupts gonadotropin signalling, and promotes visceral fat accumulation — all of which drive testosterone levels down.
This is particularly relevant if you have a waist circumference above 94 cm, a family history of type 2 diabetes, or features of metabolic syndrome (elevated triglycerides, low HDL, elevated fasting glucose, or high blood pressure).
What to do:
• Get fasting insulin, HbA1c, and a lipid panel checked — fasting glucose alone can miss early insulin resistance.
• Reduce refined carbohydrates and ultra-processed foods.
• Prioritise whole foods, adequate protein (1.6–2.2 g/kg/day), and fibre.
• Regular physical activity (especially resistance and zone 2 cardio) improves insulin sensitivity directly.
Fixing insulin resistance is one of the highest-yield interventions in all of men’s health. It doesn’t just improve testosterone — it reduces your risk of heart disease, diabetes, fatty liver, and dementia.
4. Exercise and Physical Activity
Exercise is arguably the most effective natural testosterone optimiser available. Resistance training in particular — compound lifts like squats, deadlifts, bench press, and rows — has been shown to acutely raise testosterone and growth hormone levels. Over time, the improvements in lean mass, insulin sensitivity, and body composition create a sustained hormonal benefit.
Zone 2 cardiovascular training (the kind where you can hold a conversation but it’s not exactly comfortable) improves mitochondrial function, metabolic flexibility, and cardiovascular health — all of which support hormonal wellbeing.
On the flip side, a completely sedentary lifestyle is one of the most reliable predictors of low testosterone, independent of age and body weight.
What to do:
• Aim for 3–4 sessions of resistance training per week, focusing on progressive overload.
• Include 150+ minutes per week of zone 2 cardio (brisk walking, cycling, swimming).
• Don’t overtrain — excessive endurance exercise without adequate recovery can actually suppress testosterone.
• If you’re starting from scratch, even 2–3 walks per day makes a meaningful difference.
You don’t need to train like an athlete. But you do need to move — regularly, with some intensity, and ideally with weights.

5. Alcohol and Substance Use
Alcohol is a direct gonadal toxin. Even moderate consumption (more than about 2–3 standard drinks per session, several times a week) can suppress testosterone production, increase aromatase activity, elevate oestrogen, and impair sleep architecture — compounding the hormonal damage.
Heavy or binge drinking is particularly harmful, but the relationship is dose-dependent: the more you drink, the worse the effect. Cannabis, anabolic steroids (past or present), opioids, and certain recreational drugs also have well-documented effects on the HPG axis.
What to do:
• Be honest with yourself (and your doctor) about your alcohol intake. The standard ‘couple of beers’ often turns out to be four or five when you count properly.
• If you’re drinking more than 10 standard drinks per week, reducing or eliminating alcohol is likely to improve your testosterone, sleep, body composition, and mental health simultaneously.
• If you have a history of anabolic steroid or PIED use, disclose this — it’s critical context for interpreting your blood work and planning any treatment.
Cutting back on alcohol is one of the quickest wins in men’s health. Many men notice improvements in energy, mood, and libido within 2–4 weeks of significantly reducing their intake.
6. Mental Health: Depression, Stress, and Anxiety
The relationship between mental health and testosterone is bidirectional. Low testosterone can contribute to low mood, irritability, and reduced motivation — but depression, chronic stress, and anxiety can also suppress testosterone through sustained elevation of cortisol and disruption of the HPG axis.
Cortisol deserves special mention here. It’s not just about feeling ‘stressed’ — chronic activation of the hypothalamic-pituitary-adrenal (HPA) axis directly antagonises the gonadal axis. When your body is stuck in a sustained stress response, it effectively deprioritises reproduction. This applies not only to psychological stress, but also to physiological stressors like shift work, chronic sleep disruption, chronic pain, caloric restriction, and overtraining. The result is a functional suppression of testosterone that won’t resolve until the stress load is addressed.
It’s also worth noting that many commonly prescribed psychiatric medications — particularly SSRIs, SNRIs, and antipsychotics — can affect testosterone levels, libido, and sexual function. This doesn’t mean you should stop your medication, but it does mean that any low testosterone result needs to be interpreted in the context of what you’re taking and how you’re feeling psychologically.
What to do:
• If you’re experiencing persistent low mood, anxiety, loss of interest, or difficulty coping, get a proper mental health assessment before attributing everything to testosterone.
• Identify and address your major stressors — not just the obvious ones. Shift work, overtraining, chronic pain, and financial stress all count.
• Prioritise recovery as seriously as you prioritise training: rest days, downtime, sleep, and activities that genuinely switch off the stress response.
• If you’re on psychotropic medications, discuss their potential hormonal effects with your prescriber.
• Psychological therapies (CBT, acceptance and commitment therapy) can improve both mental health and downstream hormonal function.
Sometimes what looks like a testosterone problem is really a cortisol problem — your body stuck in survival mode, with reproduction pushed to the bottom of the priority list.

7. Iron Studies and Haematology
Iron deficiency is surprisingly common in men — not just in women — and is a frequently overlooked cause of fatigue, poor concentration, reduced exercise tolerance, and even low mood. These symptoms overlap almost entirely with those of low testosterone, which is why a basic set of iron studies (ferritin, transferrin saturation, full blood count) should be part of any workup before considering TRT.
Conversely, iron overload (haemochromatosis) is worth screening for in men of Northern European descent. Excess iron can damage the pituitary gland and directly suppress testosterone production. Australia and New Zealand have some of the highest rates of hereditary haemochromatosis in the world.
There’s also a lesser-known but increasingly recognised condition called dysmetabolic iron overload syndrome (DIOS). Unlike hereditary haemochromatosis, DIOS is not caused by a genetic mutation in iron regulation — instead, it’s driven by insulin resistance and metabolic syndrome. Men with DIOS typically present with a mildly to moderately elevated ferritin (often in the 300–1000 µg/L range) but a normal or only slightly raised transferrin saturation, and HFE gene testing comes back negative. The mechanism appears to involve inflammatory upregulation of hepcidin and altered iron handling in the setting of visceral adiposity and hepatic steatosis (fatty liver).
DIOS matters in the testosterone conversation because the elevated ferritin is both a marker of underlying metabolic dysfunction and a potential contributor to oxidative stress in the testes and pituitary. Treating DIOS means treating the metabolic syndrome itself — weight loss, dietary improvement, exercise, and sometimes phlebotomy — rather than simply chasing the ferritin number in isolation.
What to do:
• Check ferritin, iron, transferrin saturation, and a full blood count.
• A ferritin below 30 µg/L is likely to cause symptoms, even if it’s technically ‘within range.’
• If ferritin is elevated (above 300 µg/L in men), screen for haemochromatosis with HFE gene testing.
• Treat iron deficiency before re-checking testosterone — you may find the fatigue resolves completely.
Don’t assume your fatigue is hormonal until you’ve ruled out the basics. Iron is cheap to test and cheap to treat.
8. Key Micronutrients: Vitamin D, Magnesium, and Zinc
These three micronutrients are singled out because they each play a direct role in testosterone synthesis, they’re commonly deficient in the general population, and they’re easy to test and correct. Deficiency in any one of them can mimic or exacerbate low testosterone symptoms — and when two or three are low simultaneously (which is common), the combined effect can be significant.
Vitamin D receptors are found in testicular tissue, and observational studies consistently show a correlation between low vitamin D levels and lower testosterone. While the evidence for supplementation directly raising testosterone is modest, correcting a frank deficiency supports overall endocrine function, energy, mood, and musculoskeletal health. This is particularly relevant in Australia and New Zealand, where despite plenty of sunshine, deficiency remains common — especially in men who work indoors, have darker skin, or live in southern latitudes (think Melbourne, Dunedin, Christchurch).
Magnesium is involved in over 300 enzymatic reactions, including those governing the HPG axis. It influences SHBG binding, free testosterone levels, and sleep quality. Magnesium deficiency is widespread — modern diets, stress, alcohol, and certain medications (particularly PPIs and diuretics) all deplete it. Symptoms of low magnesium overlap heavily with low testosterone: fatigue, muscle cramps, poor sleep, irritability, and reduced exercise performance.
Zinc plays a direct role in Leydig cell function and testosterone biosynthesis. Even mild zinc deficiency has been shown to suppress testosterone levels in otherwise healthy young men. Zinc is commonly depleted in men with poor diets, high alcohol intake, vegetarian or vegan diets, chronic gut issues, or heavy sweating. It’s also a cofactor in immune function and wound healing, so deficiency tends to show up in multiple systems.

What to do:
• Check 25-hydroxyvitamin D levels. Aim for a level above 75 nmol/L. Supplement with vitamin D3 (1000–4000 IU daily depending on your level) through winter at minimum.
• Check red blood cell (RBC) magnesium if available — serum magnesium is a poor marker. Consider supplementing with magnesium glycinate or citrate (200–400 mg elemental magnesium daily), especially if you have poor sleep or muscle cramps.
• Check serum zinc. Supplement with 15–30 mg of elemental zinc daily if deficient, and take it with food to avoid nausea. Don’t mega-dose — excessive zinc depletes copper.
• Combine vitamin D3 with vitamin K2 for optimal calcium metabolism and bone health.
None of these will single-handedly fix your testosterone, but together they form the nutritional bedrock that your endocrine system needs to function properly. And they’re among the cheapest interventions in all of medicine.
10. Prioritise Sexual Health and Your Relationship
Loss of erectile function, declining libido, and fatigue are often among the very first symptoms men notice when testosterone starts to drop — and they’re frequently the reason men seek help in the first place. These symptoms are real, they matter, and they don’t need to wait for a definitive hormonal diagnosis before being addressed. In fact, proactively optimising sexual health can improve quality of life, protect penile tissue, and support relationship wellbeing while the broader workup and lifestyle optimisation are underway.
It’s worth noting that erectile dysfunction is not just a problem of older men. Data from Hims telehealth platform showed that one in four men seeking treatment for ED is under the age of 40. ED can be an early warning sign of cardiovascular disease — the penile arteries are among the smallest in the body and are often the first to show the effects of endothelial dysfunction — but it can also reflect relational stress, performance anxiety, or the downstream effects of the metabolic and lifestyle factors covered throughout this article.
One intervention that deserves more attention is chronic low-dose PDE5 inhibitor therapy — specifically, tadalafil 5 mg daily. Tadalafil is best known as an on-demand erectile dysfunction medication, but when taken daily at a low dose, it functions more like a penile health maintenance tool. Daily tadalafil improves blood flow to the erectile tissue continuously, supporting the quality and frequency of erections (including nocturnal erections, which are critical for oxygenation and tissue health), penile length and girth maintenance, tumescence, ejaculatory control latency, and refractory period. It also helps prevent the penile trauma that can occur through repeated suboptimal erections — a process that, over time, contributes to fibrosis and further loss of function.
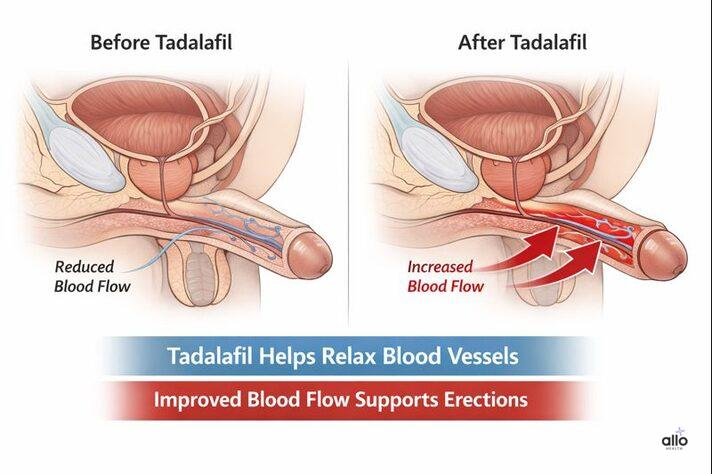
For men over 40 — particularly those noticing early changes in erectile quality — daily tadalafil can be used as a standalone intervention, alongside lifestyle changes, or in combination with TRT if hormone therapy is ultimately indicated. It’s well tolerated, inexpensive as a generic, and has additional benefits for lower urinary tract symptoms (a common complaint in the same age group).
But sexual health doesn’t exist in a vacuum — it’s deeply connected to the quality of your intimate relationship. Chronic relationship conflict, emotional disconnection, unresolved resentment, or a breakdown in communication can all drive low desire and sexual dysfunction, independent of hormone levels. Optimising sexual function with medication and lifestyle changes is important, but so is investing in the relationship itself: improving communication, resolving conflicts, and rebuilding intimacy. For some men, this means couples counselling or sex therapy — evidence-based interventions with strong outcomes that are not a sign of failure.
What to do:
• Don’t ignore early changes in erectile function, libido, or ejaculatory control — these are treatable symptoms, not an inevitable part of ageing.
• Ask your doctor about daily tadalafil 5 mg, particularly if you’re over 40. It can be used prior to, alongside, or independent of TRT.
• If you have ED, get a cardiovascular risk assessment — erectile dysfunction can precede a cardiac event by 3–5 years.
• Invest in your relationship: improve communication, address unresolved conflict, and prioritise emotional and physical intimacy. Consider couples counselling or sex therapy if needed.
• If there’s a specific sexual concern — erectile dysfunction, premature ejaculation, mismatched desire — seek help from a clinician experienced in sexual medicine. These issues are common, treatable, and nothing to be embarrassed about.
Sexual health is not a luxury — it’s a clinical priority. Optimising erectile function, addressing relational challenges, and maintaining penile health are things you can and should do now, not after a testosterone result comes back. A good sex life supports a good relationship, and a good relationship supports everything else.

10. Environmental Endocrine Disruptors
This is the issue that’s hardest to quantify individually but increasingly difficult to ignore at a population level. Endocrine-disrupting chemicals (EDCs) — including bisphenol A (BPA), phthalates, per- and polyfluoroalkyl substances (PFAS), pesticides, and certain heavy metals — are ubiquitous in modern life. They’re in plastics, food packaging, receipts, personal care products, non-stick cookware, and drinking water.
EDCs can interfere with testosterone production and signalling through multiple mechanisms: mimicking oestrogen, blocking androgen receptors, disrupting steroidogenic enzymes, and interfering with HPG axis feedback. The effects are typically subtle at an individual exposure level, but cumulative exposure over years — from multiple sources, starting in utero — is thought to contribute to the well-documented population-level decline in male testosterone levels observed over recent decades.
In Australia and New Zealand, PFAS contamination from firefighting foams at military and airport sites has been a significant public health concern, with several communities affected. More broadly, anyone living a modern lifestyle has some degree of EDC exposure.
What to do:
• Reduce plastic use where practical: avoid heating food in plastic containers, use glass or stainless steel for storage and drinking, and avoid cling wrap in direct contact with hot food.
• Choose fresh, whole foods over ultra-processed products (which tend to have higher EDC contamination from packaging and processing).
• Filter your drinking water — a quality activated carbon or reverse osmosis filter can reduce many common contaminants.
• Switch to fragrance-free, phthalate-free personal care products where possible.
• Be pragmatic, not paranoid. You can’t eliminate all exposure, but reducing the big sources — plastics, processed food, unfiltered water — is a sensible move for overall health, not just hormones.
You can’t control every chemical you’re exposed to, but you can control the biggest contributors. Think of it as reducing the background noise so your hormonal signals can be heard more clearly.
The Bottom Line
TRT can be a genuinely life-changing intervention for men with confirmed hypogonadism. But testosterone is not a shortcut around the fundamentals of good health. Sleep, body composition, metabolic fitness, mental health, substance use, and the quality of your relationships all have direct, measurable effects on your hormonal profile.
Optimising these areas first does two things: it may resolve your symptoms without the need for lifelong hormone therapy, and if TRT is ultimately indicated, it ensures you respond to treatment as well as possible.
If you’re experiencing symptoms of low testosterone, the best first step is a thorough assessment — not just a blood test, but a conversation about your sleep, lifestyle, mental health, medications, and relationships. From there, you and your doctor can make an informed, evidence-based decision about whether TRT is the right path for you.

