
Most blokes with back pain end up on one of two tracks: physio forever, or a surgeon's waiting list. There's a middle option your GP might not mention — and it's probably bulk-billed.
If you've been grinding through back pain for months — tried the physio, done the stretches, swallowed the anti-inflammatories — you've probably hit the point where someone says the S-word. Surgery.
But here's the thing most people don't realise: there's a whole category of targeted, image-guided procedures that sit between "keep doing your exercises" and "let's open you up." They're performed by interventional radiologists — doctors who specialise in using real-time imaging to guide needles to the exact spot causing your pain.
No general anaesthetic. No overnight stay. No six-week recovery. And in Australia, most of these procedures are bulk-billed under Medicare.
The catch? Your GP might not think to refer you for one. Not because they don't care — but because this pathway doesn't get the airtime it deserves. So here's what you need to know, and what to ask for.
First: What Kind of Back Pain Are We Talking About?
Not all back pain is the same, and the treatment depends on which flavour you've got. Broadly, it splits into two patterns.
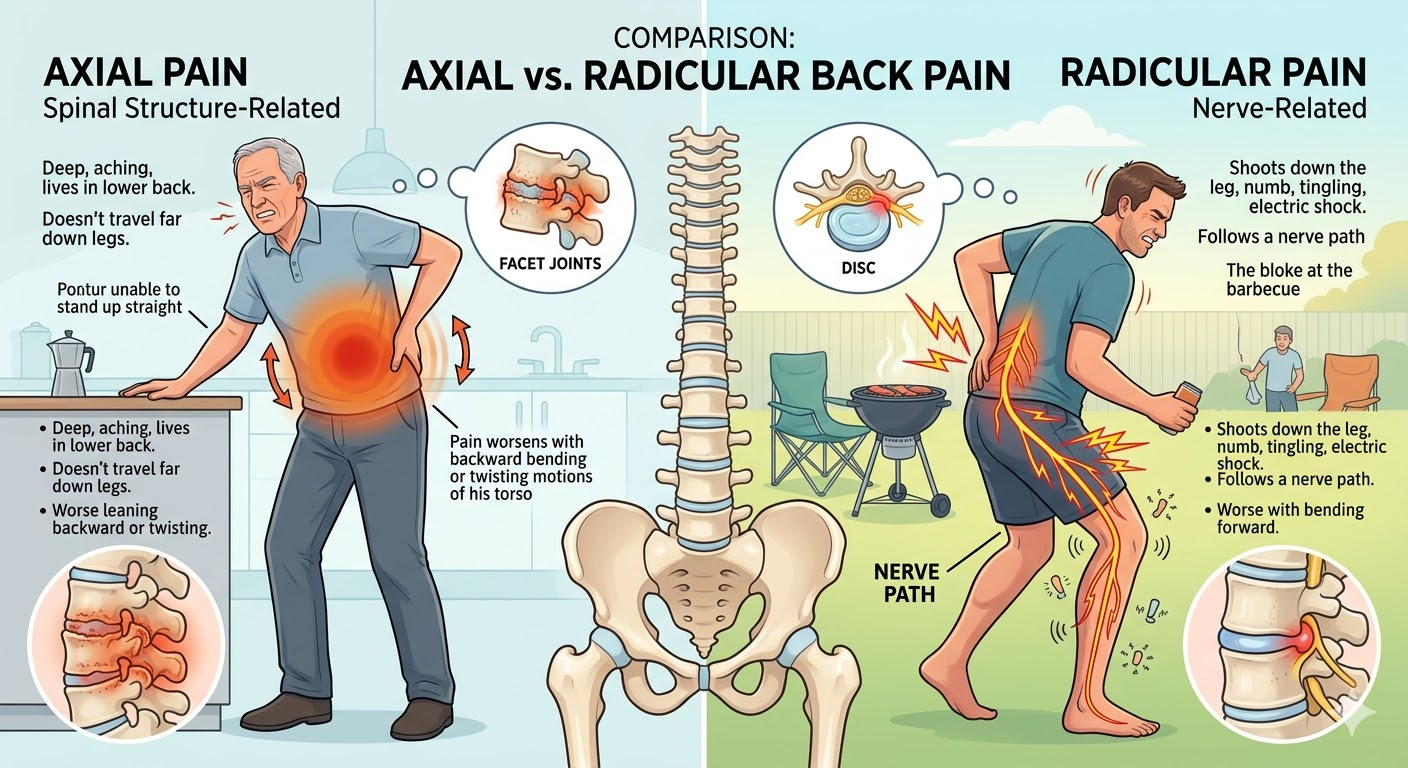
Radicular pain is when the pain shoots down your leg — sometimes with numbness, tingling, or that electric-shock feeling. It follows a nerve path, usually below the knee, and it's typically worse when you bend forward. You know the bloke at the barbecue who can't sit in a camp chair without shifting every thirty seconds? That's often radicular pain. It usually means a disc is pressing on a nerve, or something is narrowing the space where the nerve exits the spine.
Axial pain is the deep, aching, "I can't stand up straight" kind. It lives in your lower back, doesn't travel far down the legs, and often gets worse when you lean backward or twist. It's the pain that makes you brace against the kitchen bench when you've been standing too long. This usually points to the facet joints — the small paired joints that link your vertebrae together — wearing out or getting inflamed over years of use.
Your GP can often tell which pattern you've got from a good history and examination. An MRI confirms it. And the type of pain determines which procedure you'd be referred for.
The Procedures: What Actually Happens
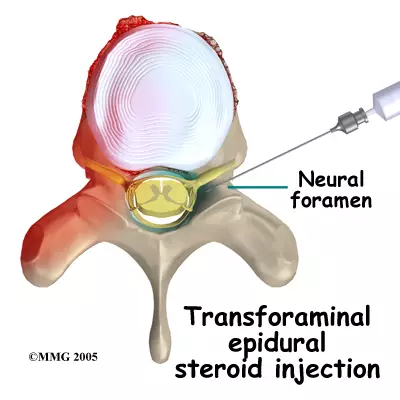
Transforaminal Epidural Steroid Injection (for nerve pain down the leg)
This is the workhorse for radicular pain. A radiologist uses live X-ray (fluoroscopy) to guide a thin needle to the exact nerve root that's being compressed. They inject a small amount of anti-inflammatory steroid directly where the inflammation is worst.
On the day: You lie face-down on a procedure table. Local anaesthetic numbs the skin. The radiologist uses real-time imaging to position the needle — you might feel pressure but not sharp pain. The whole thing takes 15 to 30 minutes. You go home the same day. Most people are back to normal activity within 24 to 48 hours.
What to expect: Around 60 to 80 percent of people get meaningful pain relief. For some, it lasts months or even years. For others, it buys enough time for the disc to settle down on its own — which many do.
The key advantage over surgery: It's reversible. If it doesn't work, you haven't burned any bridges. If it does, you may have avoided an operation entirely.
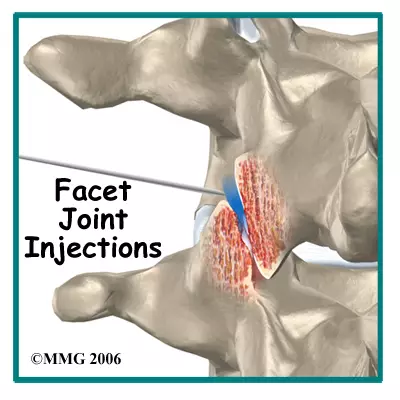
Facet Joint Injections and Medial Branch Blocks (for deep back pain)
If your pain is axial — centred in your lower back, worse when you extend or twist — the facet joints are often the culprit. These are small paired joints that sit behind the disc at every level of your spine, and they cop a lot of wear over the years.
The approach here is a two-step process. First, the radiologist injects local anaesthetic around the tiny nerves (medial branches) that supply the facet joint. This is a diagnostic block — essentially a test. If your pain disappears for a few hours, it confirms the facet joints are the source.
If it works on two separate occasions, you're a candidate for radiofrequency ablation (RFA) — where the radiologist uses a needle to heat and disable those same tiny nerves. The joint is still there, but the pain signal gets switched off.
On the day: Similar setup to the epidural — face-down, local anaesthetic, image-guided needle placement. RFA takes a bit longer (30 to 45 minutes) because multiple nerves are treated. You go home the same day.
What to expect: RFA typically gives six to twelve months of relief. The nerves eventually regenerate, but the procedure can be repeated. Some people get years of cumulative benefit from periodic treatments.
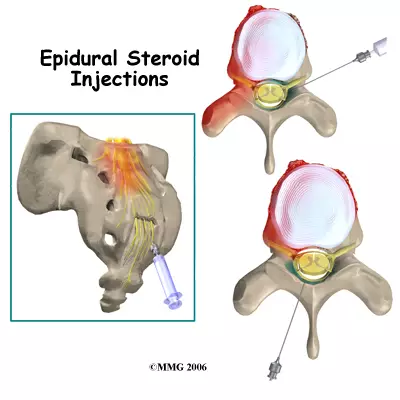
Interlaminar Epidural (for spinal canal narrowing)
If your MRI shows central canal stenosis — the main spinal canal narrowing and squeezing multiple nerves — a slightly different approach is used. Instead of targeting a single nerve root, the radiologist delivers steroid into the central epidural space, bathing the compressed area more broadly.
This is particularly useful for people who get leg pain and heaviness when they stand or walk, but feel better when they sit down or lean forward (neurogenic claudication). It can buy significant time, especially for people who aren't keen on — or aren't fit enough for — decompression surgery.
Synovial Cyst Puncture (the one nobody's heard of)
Occasionally, a fluid-filled cyst grows from a facet joint and presses directly on a nerve. It looks dramatic on the MRI but the fix can be straightforward: the radiologist punctures the cyst under image guidance, deflates it, and injects steroid to reduce the chance of recurrence.
Most people have never heard of this option and end up on a surgical waiting list for something that can be sorted in 20 minutes with a needle.
Why a Radiologist and Not a Surgeon?
This isn't about one specialty being "better" than another. It's about matching the right tool to the right problem at the right time.
Most people think of radiologists as the doctors who read their scans. And they do. But interventional radiologists are a subspecialty who spend their careers guiding needles and catheters under real-time imaging — fluoroscopy, CT, ultrasound. That precision matters when you're placing a needle millimetres from a spinal nerve. They're not competing with surgeons; they're filling a gap in the pathway that often gets skipped.
The gap exists partly because of how referral patterns developed in Australia. For decades, the default pathway for persistent back pain has been GP → physio → orthopaedic surgeon or neurosurgeon. Interventional radiology grew up in a different lane (think angiograms and biopsies) and the spine work is relatively newer on the radar for many GPs. That's changing, but slowly.
Surgery is still the right call for some people — particularly if there's structural instability, severe compression causing weakness, or nerve damage that's getting worse. But for the majority of back pain presentations, a targeted injection or ablation is a reasonable — and far less invasive — first step.
The practical comparison:
- IR procedure: Local anaesthetic, 15–30 minutes, home same day, back to work in 48 hours, bulk-billed under Medicare.
- Spinal surgery: General anaesthetic, 1–2 hours, overnight stay minimum, 2–6 weeks recovery, several thousand dollars out-of-pocket if private (or months on a public waiting list).
If the injection works, you've avoided surgery. If it doesn't, you've lost nothing — and the surgeon still has all the same options available.
The Best Imaging to Get Before Your Referral
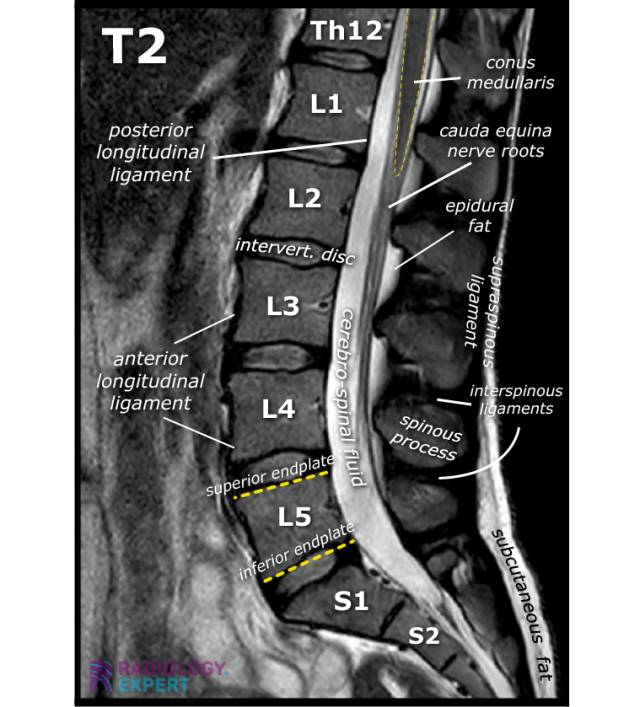
An MRI of the lumbar spine is the gold standard. It shows discs, nerves, facet joints, cysts, and the spinal canal in detail — without any radiation. This is what the radiologist needs to plan the procedure.
A plain X-ray is useful for checking alignment and bony changes but won't show soft tissue detail. CT is good for bone but misses disc and nerve detail that MRI picks up. If your GP is sending you for imaging, push for the MRI — it's the one that actually drives the treatment decision.
One caveat: if you have a pacemaker or certain metallic implants, MRI may not be suitable. Your GP and radiologist will work that out.
But MRI doesn't change management, does it?
They're not wrong — but they're not completely right either. The "MRI doesn't change management" line comes from solid evidence that for acute back pain (under six weeks, no red flags), early imaging doesn't improve outcomes and can lead to unnecessary worry about findings that were never causing the problem. That's good medicine.
But the conversation changes once someone has done the conservative work — six to twelve weeks of physio, activity modification, appropriate pain relief — and they're still significantly limited. At that point, an MRI isn't fishing for trouble. It's answering a specific clinical question: is there a structural target that an interventional radiologist can treat?
A disc compressing a nerve root, a facet joint cyst, multilevel canal stenosis — these are findings that directly determine whether a targeted, bulk-billed procedure could shortcut months of ongoing pain. The MRI doesn't replace conservative management. It's what comes next when conservative management has had a fair go and hasn't got the job done.
What to Ask Your GP to Include on the Referral
This is where you can genuinely help move things along. When your GP writes the referral to an interventional radiologist, the more specific the information, the faster and smoother the process. Ask them to include:
- Your pain pattern — is it leg-dominant (radicular) or back-dominant (axial)? How long has it been going on? What makes it worse?
- What you've already tried — physio, medications, previous injections. This tells the radiologist you've been through conservative management appropriately.
- The MRI findings — specifically which level and side the pathology is at (e.g., "L4/5 right paracentral disc protrusion with traversing nerve root compression").
- What you're hoping for — diagnostic block to confirm the pain source? Therapeutic injection for relief? Consideration for RFA? Being explicit about the question helps the radiologist plan the right procedure.
If your GP isn't sure which procedure to request, that's fine — a referral that says "please assess for image-guided intervention" with the clinical details and MRI report attached is enough for the radiologist to take it from there.
What If It Doesn't Work?
Worth addressing, because nothing works for everyone. If the injection gives you less than 50 percent relief, or the benefit wears off quickly, that's still useful information. It helps narrow down where the pain is actually coming from — and it tells your team whether the next step is a different injection target, a different approach, or whether surgery genuinely is the best option.
The point is: trying an IR procedure first doesn't delay anything meaningful. You get an answer within days to weeks, not months. And if the answer is "this isn't the right fix," the surgical pathway is still fully open.
The Bottom Line
Back pain is one of the most common reasons Australians see their GP, and one of the most common reasons people end up frustrated. The pathway from "physio isn't cutting it anymore" to "I guess I need surgery" skips an entire step — one that's minimally invasive, evidence-based, and often free under Medicare.
You don't need to be a medical expert to ask the question. Next time you're in with your GP, try: "Before we talk about a surgeon, can we look at whether an interventional radiologist could help?"
It might be the most useful sentence you say all year.

